



An explanation of The Posture Theory diagram
© designed in 1980

The Posture Theory diagram summarises an idea that took five years to develop (between 1975 and 1980) and it aims to give an instant, and reasonable understanding of the concept.
It depicts a man sitting at a desk and leaning forward to read.
The left side of the diagram contains straight dashed lines and a curved line which show the movements that occur when leaning forward, and the external pressures that are created.
The large dot in the middle represents the position just below the tip of the breastbone, and is like an axle about which the upper body rotates when the person leans forward and backward while slouched at the waist.
The lines inside the man are there to give an impression of the way mechanical pressure affects internal structures as he leans forward.
The column of words on the right side show the sort of symptoms that can result.
The angles of pressure
The vertical line in the middle represents a position parallel to the spine when the person is sitting upright. The next line to the left of it represents the distance that a particular individual leans his head and shoulders forward if he has a stooped spine or a slouch. The angle between the two lines is called the stoop angle.The next line represents the extra distance he would lean forward to get his eyes close enough to a page so that he could read the text. He will naturally sit up after he has read the text, and lean forward when he needs to read or write again, so it is called the angle of oscillation, i.e. the angle made as he repeatedly leans to and fro about that axis. The final line from the axis to a position in front of his feet is used to show how much relative pressure is created by leaning forward. It is an inverse angle because the worse a persons stoop, and the more they lean forward, the greater the pressure, and the smaller that angle will be. Another way of determining the amount of pressure could be to add the stoop angle and the angle of oscillation, in which case the larger the angle, the greater the pressure.
The list of symptoms in the diagram
The words to the right of the man in the diagram above show the various effects of postural pressure on the spine and internal organs, starting at the top with “distortion of sinus cavities and ducts“. When the head is upright and the neck is vertical the air passes freely through the nose and down the windpipe. However any forward or backward bending of the neck alters the angles and pressures at the top of the throat and disposes to inflammations and swellings, and congestion of the ducts or tubes in that area, such as nasal congestion. The distortion is more pronounced when the neck is stooped forward, and the person lifts their head to talk to someone directly in front of them.
Similarly with the spine bent forward the neck pushes the lower jaw bone forward, which in turn pushes the lower teeth forward against the upper teeth which is a type of ‘clenching’ of the teeth that can cause deformities to the shape and position of the teeth, especially in growing children. It can also cause tenderness in the gums and strain on the jaw joint which may result in referred pains to parts of the face.
When the spine is stooped forward and the is head tilted up and back the extra bend in the neck puts abnormal pressure on the discs in the middle section of the neck, and strains the muscles, ligaments, and nerves in that area, which disposes to neck ache and possibly contributes to headaches. The middle bones of the neck also push forward which stretches and compresses the front of the throat, and disposes to tenderness or sore throat and colds. The forward and, or backward movement also affects the larynx or ‘voice box’, and can cause voice problems, as in hunchbacks who tend to talk in a husky fashion. That pressure can also affect other structures such as the Eustachian tubes which lead to the ears, and, the valve like junction which separates the foodpipe from the windpipe.
(You can slouch forward, and then move your own head forward and back to feel some of the effects temporarily for yourself, and try pushing your head all the way back until you can feel the pressure under the back of your head, and the stretching of your throat, and then push your chin down and back toward your neck until you can feel the pressures at the top of your throat. It won’t become a problem unless you have a permanent stoop, or constantly sit in an unhealthy slouched position).
More obviously, when the shoulders are slumped forward they go over and above the chest causing the weight of the head and shoulders to press down on the cavity in the chest, which contains the heart, lungs and breathing muscles. The pressure on the heart can make the heartbeat more easily felt and dispose to palpitations, and pressure on the breathing muscles can cause them to cramp, and also impair the upward movement of the diaphragm so that the breathing requires more energy and is shallower and less efficient. The shallow breathing can cause a stagnation of some of the air in the lobes of the lungs and dispose to lung infections.
(You could gain some understanding of this by forcing yourself to do deep breaths while you are in a relaxed upright posture, and then when you are in a forced slouch, and feel the differences i.e. when you are sitting upright, and you inhale, your diaphragm will rise up into your chest and your chest will expand outwards, but when you are in a forced slouch your diaphragm will rise to your lower ribs and stop. You will then feel upwards and outwards pressure in that area, and your upper abdomen will expand outwards, but your chest won’t move).
The pressure on the air in the chest can act like a tourniquet and impede the flow of blood from the feet to the heart, and through the chest to the brain to cause difficulty concentrating, or thinking, faintness, tiredness, and fatigue.
The forward movement of the head also pushes the weight of the shoulders over and above the twelve sets of ribs at the front of the chest.
That pressure puts strain on the structures between them, which become tender, especially between the lower ribs of the right side, but sometimes on the left and in other areas. The person may not be aware of any soreness unless they press on the tender spots with their fingers, or unless they get occasional sharp stabbing pains in those areas (like a pinched nerve).
The forward position of the shoulders can also dispose to mild or severe cramps in the muscles at the far left and right side of the chest.

The chest also contains a breastbone in front, which has the shape of a broad dagger with a blunt tip. In people with flat chests who lean forward from the waist (instead of the hips) the broad part presses backwards and compress the heart, lungs, and air in the chest, which increases the effect of the downward pressure from the shoulders.
The tip of such a breastbone would also press into the general area where the foodpipe joins the stomach, which can affect the efficiency of the valve like structure between them and cause some backflow or reflux of stomach acid. The upward flow of acid can make the inside of the foodpipe sore and tender, and the pressure and irritation can cause spasm of the junction which is called esophogeal achalasia (more accurately a failure of that section to relax properly).The tip of the breastbone also stabs into the area of the solar plexus which is a bundle of nerves that controls many abdominal functions.
The forward leaning also pushes the lower ribs downwards to press on the colon which is a long tubular structure that carries food residue from the stomach to the rectum. A section of that tube goes up the left side of the abdomen, across the top, and down the right side. The lower ribs tend to press on the bends on the left and right side, and in other sections to impair the flow of material which disposes to irregularity, constipation, and spasm of the colon, and to blockage of the appendix and appendicitis, and to the formation of small pressure ruptures or pouches in the colon wall called diverticula, which may become infected to cause diverticulitis.
The rounded curve of the back also places strain on the muscles of the mid spine, and pressure on the kidneys which filter used blood to produce clean blood and urine. Pressure on the kidney can impede the blood flow and the filtering process and may be a cause of an excessive concentration of salts which results in kidney stones. Pressure on the adrenal glands which sit on top of the kidneys may contribute to unstable or high blood pressure and an irregular or excessive output of adrenalin, and general secondary irritability of the nervous system.
When sitting upright the weight of the head and chest is transferred evenly down the bones of the spine, but when leaning forward the muscles of the lower spine are stretched, and take some of the weight, which disposes to aching in the lower back.
Treatment: The most practical and effective way of relieving all of those symptoms, which I developed gradually over a period of thirty years, was to go from a sitting and writing position, to standing and typing at a computer, with the keyboard at waist height, and the screen at eye height, so that it isn’t necessary to lean forwards. See here. Other practical and useful methods which I studied and used are discussed elsewhere on this website. e.g. see here M.B.
A reference for the measurements of pressure on internal cavities: On November 5th 1887 The New York Medical Journal included a study of scientific measurements of the pressure created on the internal anatomy by corsets and posture. Some relevant information can be seen by scrolling down to Figure 15 here
Female movie stars will often report how breathless and exhausted they were when wearing corsets as part of their role in movies about nineteenth century society, and they report how glad they were to get out of the corset so that they can breath properly again.
Some more experiments to test the effects of postural or other mechanical pressures on the human body:
You could try breathing while a belt is strapped tightly around your waist or chest, or your could try wearing a tie around
your neck which is extremely tight, or you could put a blood pressure cuff on your arm and pump it up with air until the flow of blood to your hand stops and you start feeling a sensation of pins and needles in your fingers, or you could apply a very tight garter, or a tight rubber strap around your leg. Prolonged use of leg garters can cause varicose veins.
As you can appreciate, if tight collars can block blood flow through the neck , and tight garters can block blood flow to and from the feet, then tight belts, girdles, or corsets around the waist can block blood flow between the feet and the brain, and postural pressure on the abdomen can have the same effect.
When doing the experiments described in this essay, bear in mind that the effects will vary from person to person because the shape of the spine and the shape of the chest will determine the angles of pressure and the effect on your body. Such differences are discussed in more detali in other parts of this website.
Types of posture ©
1. Good posture involves an upright spine with slight natural forward curves in the neck and lower spine, and broad and straight shoulders. Significant increases in the curves or other changes in shape are listed below.
2 . Poor posture is the term used to describe an abnormal forward curve in the upper spine due to slouching while standing, and a C-shaped curve along the entire spine which can be seen from the side when a person slouches forward in the sitting position. Hence it is often referred to as the slouched posture.
3 . Kyphosis is a more extreme forward curvature of the upper spine and is due to an abnormality in the structure of the spine and is generally referred to as the hunchback posture. It is usually accompanied by a corresponding forward curve in the lower spine so that it looks like a reverse S-shape when seen from the side.
4 . Scoliosis is the medical term for sideways curvature of the spine which usually results from a person using one hand to do most of their tasks because most people are either left or right handed. it can also result from one leg being longer than the other. See a scoliosis X-ray here

5 . Lordosis is an excessive forward curve in the lower spine and is usually associated with a hunchback posture. Common causes are obesity or pregnancy where the weight of the abdomen drags the lower spine forward.
6 .Swayback is the backward curvature of the lower spine
7 . Flatback is where the normal slight curves of the spine are not present and the back is abnormally straight.
8 . Kypholordosis is the combined abnormality of a forward stoop in the upper spine (kyphosis), and a forward curvature of the spine (lordosis), and usually occurs because the stoop puts the weight of the persons head in front of the centre of gravity with a tendency to fall forwards, so the instinctively push their lower spine forward to restore the centre of gravity and maintain a counterbalance upright position. A side view of the body shows a spinal colum with an S-shape.
9 .Kyphoscoliosis the combination of a forward curvature of the upper spine (kyphosis), and a sideways curvature (scoliosis), where multiple abnormalities commonly occur because they may be due to poor nutrition which weakens the bones or muscles, and affects every part of the human skeleton in a variety of ways.
10 . Kyphocostosis is the combination of forward curvature of the upper spine (kyphosis), and deformities of the rib cage (costosis) which involves abnormalities of the chest, such as one that is abnormally flat and shallow, or deep and barrel shaped.
11. Neck stoop can be seen from the side view in a person with a deep chest where the rib cage forms a triangular structure which prevents the spine from collapsing into a C-shape, so it remains straight, but the neck bends sharply forwards.
This information was first posted on 1-1-11 and most of it is derived from my book published between 1994 and 2000
Diagnosis of postural problems ©
The following suggestions give a concise summary of how to diagnose the different types of posture abnormalities.
Most people have mild postural problems but are not aware of them because they generally only see themselves from the front view in the mirror, but, for example, the forward slouch is only obvious when viewed from the side.
1. Forward curvature of the upper spine can be identified by looking at the way a shirt or a coat hangs on the shoulders. If the person is sitting with an upright spine the shirt will hang flat. However if they have a slouch or a stoop the cloth may be wrinkled into folds. The forward curve can then be seen by looking at the person from the side view. Another clue can be seen in their tendency to support their head by having their elbow on a table, and their hand on their chin. They will also look smaller when sitting slumped in a chair, compared to people of the same height who sit upright. If you look at them from the side view the curvature in the upper spine will be obvious.
2. Sideways curvature of the spine can be identified by looking at the person from the front view and noticing that one shoulder is lower than the other. Also the highest shoulder will be parallel to the ground, whereas the lower shoulder will be angled downwards. The persons shirt collar will be lower on one side, and their clothes such as their coat will hang lower on one side. If they take their shirt off you will be able to see that one collar bone is lower than the other, and slopes downwards, and if you feel their Sternum bone from top to bottom well notice that it is tilted sideways. If the person is viewed from behind in the sitting position while they are leaning forward with their elbows on their knees, one side of the shoulder will look normal, but the other side will roll significantly downwards at an angle that can be easily seen to be abnormal.
3. Lordosis is usually easy to identify by the cause. For example, if a woman is pregnant and the womb is large, her belly will be heavy and protruding forward, so the forward curve of the lower spine will exist and can be easily seen from the side view. Similarly an overweight or obese person will probably have a heavy belly which drags the lower spine forward. Also if there is a forward curvature of the lower spine from other causes it will push the abdomen forward to produce a pot bellied appearance.
4. Flatback can be seen from the side where it looks as if the person has a steel rod for a spine, rather than a series of vertebrae that form a slight natural S-shape.
5. Kypholordosis is forward curvature of the upper spine with a corresponding forward curve in the lower spine which often involves chest abnormalities as well, and leaves a crease line across the skin of the abdomen just below the ribs, and the person will appear to have a small pot belly. When viewed from the side the spine has an S-shape.
This information was first posted on 1-1-11 and most of it is derived from my book published between 1994 and 2000
See also posture assessment charts or grids on this video here
The prevention and treatment of posture related problems
Prevention is better than cure
Poor posture is unlikely to cause problems such as back pain in the first few years of life, but it can have a more serious effect if it gradually changes the shape of the spine and becomes permanent as the child develops into adult hood. Knowing how to prevent the problem is also useful at any stage in relieving or managing the secondary symptoms.
Poor nutrition affects the strength of the muscles and bones that support the human posture, so good nutrition is important. Similarly any infectious illness that results in nausea, vomiting, diarrhea, poor appetite, and weight loss can weaken muscles and bones so they should be guarded against, and recovery from them should include the appropriate type of exercise to regain strength as soon as possible, especially during childhood.
Other preventive measures include sleeping on bedding that is flat and has the degree of firmness that allows the natural slightly S-shaped curve of the spine to be maintained. e.g. not so hard that the spine is kept too straight, and not so soft that it sags like a hammock. Many bedding companies provide advice on such requirements.
It is important to use appropriate seating for the persons size. The height should be such that the feet can be placed flat on the floor for support. The length of the chair should be in proportion to the length of the thigh so that the lower back is not dragged forward into a curve, and the back rest of the chair should be slightly inclined backwards, and have a slight curve in the mid to lower back area to support that natural slight curve in the lower spine.

The angled platform of a seventeenth century scribe would reduce the need to lean forward, but note the man’s stooped shoulders.
That my be related to the fact that he couldn’t move his knees forward, so his lower spine was positioned away from the bench.
When sitting at a desk it should be at a height that the person does not have to lean forward to read, and if the person does lean, they should do so from the hips and not the waist. Writing requires the use of one hand and movements to the left and right side of the page which twists the spine and breastbone, so it is preferable to use computer keyboards which require both hands equally and do not result in twisting the spine. The keyboard and mouse should be level with the forearm when it is parallel to the ground so as not to bend the wrist which can interfere with blood supply to the hand. The computer screen should be at eye height. In general any activity that requires leaning toward a desk should be avoided, but ordinary sitting without leaning forward is not such a problem. If it is the person can use a properly designed recliner chair to rest in and relieve some of the aches that result from postural strains during the day.
For an illustration about computer posture from another website see here
Children who carry heavy school books to and from school in satchels or kit bags may develop sideways curvature of the spine, so they should avoid carrying unnecessarily heavy books, and put them in knapsacks on their backs instead. Similarly, having one leg longer than the other can cause sideways curvature of the spine, but that can be remedied by the use of shoe inserts, and some practitioners specialise in that aspect, and, in some cases orthopedic surgeons can lengthen the short leg. Women should avoid wearing high heel shoes because they lift the heel, and tilt the hip bone, and push the abdomen forward, and curve the upper spine into a stoop. If they still want to wear them they should consider that occasional use in social situations is better than wearing them all the time.
There are numerous other methods, but it is also important to know what normal posture is, and what defects you may have. This can be assessed by looking sideways into a mirror to determine if the spine is abnormally stooped or S-shaped, and by looking front on to see if one shoulder is lower than the other, indicating sideways curvature of the spine.
Throughout history there have been many observations about the harmful effects of poor posture and many methods have been devised to relieve the problems. The most obvious is Yoga, but there are others such as chiropractic and osteopathy, and more recently the Alexander Technique which partly involves raising the head so that the spine straightens out, and then finding a position of balance where the head is directly above the spine and feet so that good posture can be maintained by balance, rather than by straining the muscles to stop the body from falling forward or backwards. Physiotherapists now incorporate some of those methods in their practice, and if deformity is severe it can sometimes be treated by orthopedic surgeons.
Education about the benefits of good posture is perhaps the most important.
Some notes on using braces and straps to correct postural problems
Braces are not a practical treatment for spinal deformities because they can’t correct the curve and can weaken the musculature.
Reference: The Specialties in General Practice (1951) p.72-74.
My comment: There are a number of problems associated with wearing spinal straps or braces to straighten the spine. Firstly some people will have other injuries and pains caused by their poor posture, and the brace can make them worse. Secondly wearing them supports the spine, so the spinal muscles don’t have to carry the weight of the body and will therefore weaken due to lack of use.
Nevertheless, some people might find them an advantage. Perhaps wearing them occasionally to ‘train’ the person to adopt a particular posture may be beneficial. For example, in young people with pliable spines, if the brace is worn for a few hours a day, it might gradually straighten the bones, and if they then remove the brace, but maintain that general posture with their musculature for the remainder of the day they may gain some effective improvement in spinal shape without losing muscle tone, and consequently avoid having the problem return. However, it is not something for me to comment on other than that. The Alexander Technique is another way to improve posture, and shoe inserts etc. can correct spinal curvatures which are due to having one leg shorter than the other, or to deal with spinal problems associated with abnormalities of the feet. Other methods such as yoga, osteopathy, and physiotherapy etc. are available.
In general terms – the treatment needs to be tailored to each patient, and what works for one might not be effective in another, and prevention and early treatment are the best options.
The importance of early treatment and correction of postural deformities

“It is important that this treatment should begin as soon as possible; if a curvature is allowed to persist for some time the shape of the bones may alter and there can then be little hope of correcting the deformity.” Reference: The Illustrated Family Doctor, 1935, page 620.
People who attribute poor posture to a bad habit, or to psychological factors such as anxiety, or depression, are essentially “blaming the victim” for the failure of treatment. Many treatments may have the best of intentions, and may have some useful benefit, but they can’t and won’t change the shape of the bones of the spine, which is the real cause of the persistent stoop. It is not ethical for adults to be blaming small children for problems which should have been prevented and treated early. Poor posture is a purely physical problem that needs to be studied and treated as such. Psychological problems may or may not be involved in individual cases but are essentially irrelevant and should be treated as a completely separate issue but only if they exist as an accompanying or purely coincidental aspect.
Some notes on education
1. Charles Darwin once said that the human body is covered by a layer of skin and hence the average man knows no more about it’s inner workings than he does about the inside of a ship, and a nineteenth century physician said that only the anatomist knows the horrendous effects that corsets have on distorting the shape of internal organs. Of course, an anatomist slices open the skin and looks inside, and could see that, in some cases, the spleen had been pushed from the top left of the abdomen to below the navel, and the liver had been split almost in two, and the woman would be complaining about horrendous aches and pains, and the corset industry would argue that corsets were not the cause because the woman still had a spleen and still had a liver???? The corset industry lost
2. Most people are not aware of the effect poor posture has on internal anatomy, and won’t unless they are educated about the topic
3.. When you look at the sky with your eyes it looks as though the sun rises in the morning and goes down at night. If you use your brains it doesn’t.
4.. Never judge a man until you have walked in his shoes. There may be a few tacks that are digging into his flesh and bones with every step that he takes, but his shoes may look as comfortable as lounge room slippers.
Treatment options
Foot and posture treatment: Rothbart’s foot
Braces and straps: PostureJac
Surgery: YouTube video on the surgical correction of stooped and sideways curvature of the spine here
Prevention: Ergonomics
For an interesting video on posture improvement principles see here
The causes of poor posture
As a general rule medical conditions cannot be prevented or treated effectively unless the correct cause is known, and as the old saying goes “prevention is better than cure”.
While I was looking for the causes of spinal deformities I often found these comments in medical books.
Hunchback is associated with sideways curvature of the spine where it may be due to polio, tuberculosis of the spine, or in old age osteoporosis. However, in three quarters of cases the cause is unknown . Reference The Marshall Cavendish Illustrated Encyclopedia of Family Health (1988).
In 85% of cases of scoliosis (sideways curvature of the spine) the cause is obscure. Of the remainder 10% follow poliomyelitis, 2% due to VonRecklinghausen’s disease or neurofibromatosis, and less than 2% are due to congenital bone disorders in the spine, osteochondrodystrophy, Freidreic’s ataxia, cerebral palsy, and some muscular dystrophies, Also less than 2% follow empyema, thoracoplasty, or any other factors which change the chest shape during the growth period.
95% of cases are girls, usually starting at the age of 10, although occasionally earlier, and increasing gradually to the age of 15, and the degree of curve does not increase after the age of 15. There is still considerable controversy in the whole field of scoliosis. Reference: The Specialties in General Practice (1951) p.72-74. See also a modern reference from 2006 here.
See also a modern reference from 2006 here.
Consequently while I was studying the subject I was looking for and identifying the other 85% of cases, the majority of which are generally due to long term biomechanical factors, and can be seen in the list below .
Corset Design Stoop
In previous centuries women have changed the shape of their bodies by wearing corsets. In fact, the manufacturers of corsets designed them to produce a particular shape to suit the fashion of the time. While they were known to be tight at the waist (e.g. to produce the hour glass shape), they were also designed to alter the shape of the spine in specific ways. Some mothers provided them for their children to wear from an early age, where they were referred to as training corsets – to train the body to gradually take on that permanent shape by adulthood. Diagram Reference: The Analysis Of Beauty (1739

A list of 25 causes of poor posture, and related aspects
Banfield’s posture axiom: There are many causes of poor posture, not just one, and many health problems caused by poor posture, not just backache
| Animal Stoop | I once had a fish aquarium in which I kept small fish called guppies. They had a long narrow body, but when the females became pregnant in the first year their belly bulged downwards in the front half. They gave birth to about a dozen small fish each. However when they became pregnant in later years their belly would bulge to almost twice that size and they would develop an upturned V-shaped bend in the middle of their spine and swim about in an awkward manner. They would soon give birth to many dozens of small fish, and their bellies would return to their normal size, but the upturned V-shape in their spine remained as a permanent feature, and they continued to swim in an awkward manner. I have since noticed that women develop spinal curvatures during pregnancy, more so when having twins or triplets, and have discussed that on this list below as the Pregnancy Stoop. See also an article on the genetic factors and the spinal deformity of guppies here. Spinal problems can also occur when people try to develop different features in animals. For example the dachshund is also called a sausage dog because of it’s long narrow body and short legs. Some breeders like to produce offspring which have longer bodies than normal, but that results in the middle of the back sagging downwards particularly if the dog is overfed and becomes obese. Ultimately that deformity can lead to arthritis of the spine and back injuries. |
| Athletes posture | The size and shape of the chest determines lung capacity, and postural compression of the chest due to the hunchback posture etc, has the same effect. That in turn reduces the size or space in the lungs and the amount of oxygen a person inhales with each breath, and hence, athletes with the largest lungs are the most likely to win events, especially sprints and marathons. The same thing applies to swimmers. Consequently improving posture will improve athletic performance.See simmers posture. See also Marathon runners posture, and swimmers posture. |
| Baby Stoop | Rickets caused by a deficiency of calcium and Vitamin D in the diet, or the lack of exposure to sunlight. (Vitamin D is produced by the skin when exposed to sunlight). See here |
| Bacterial or viral stoop | A prolonged Bacterial or virall infection in childhood where there is a loss of apetite, muscle tone, and body bulk, which causes the upper spine to bend under the weight of the body. |
| Banfield’s kyphosis | An alternative label for the one which I invented and defined as “nutritional kyphosis” which is based on my assessment of the cause of my own skeletal and spinal abnormalities. See here. The nutritional aspect can be due to malnutrition, or poor apetite, nausea and vomiting associated with bacterial or viral infections in childhood. |
| Bed shape posture | Individuals sleep on beds for 8 hours or more per night, and as such the shape of the spine is likely to take on the shape of the bedding, particularly in the growing years of childhood when the bones are pliable. A mattress which is too hard is likely to flatten out the natural slight curves of the spine and may sometimes be responsible for back pain when the person wakes up in the morning. Similarly sleeping with the head resting on pillows which are too hard may cause an abnormal curvature in the neck, and or, the person to wake up with neck ache. The hammock shape may produce a C-shaped spine. Orthopedic bedding and mattresses which are designed to be flat and soft enough to absorb the weight of the head, shoulders, and hips, is more likely to retain the natural and proper shape, and prevent or relieve backaches. |
| Chair shape posture | Sitting in chairs which are the wrong shape, or are too straight at the back are likely to cause the spine to become abnormally straight, or to cause the head and shoulders to fall forward and result in slouching and spinal curvatures, where as properly designed chairs can retain the natural shape of the spine. See here |
| Chest shape stoop | A deep chest has a triangular shape when viewed from the side, and the ribs provide geometric and structural support for the spine in a manner which keeps it straight. However a flat or funnel shaped chest does not provide as much resistance to forward movement so it is likely to collapse into a stoop in response to forward pressures, particularly those on the upper spine. |
| Congenital stoop | Congenital dislocation of the hip can cause forward curvature of the upper spine (kyphosis). |
| Corset Design Stoop | The shape of the corset especially one which is worn on a regular basis during childhood for the purpose of permanently changing the shape of the waist and the spine to suit the fashion of the period. |
| Da Costa’s syndrome posture | The symptoms of Da Costa’s syndrome include chest pains, palpitations, breathlessness, faintness, fatigue, and abdominal pains etc. The typical patients has a thin and stooped physique and a long, narrow, or flat chest, and is a poor athlete and a poor swimmer. |
| Darkroom Stoop | Vitamin D deficiency of rickets due to a lack of exposure to sunshine during childhood etc.. |
| Dentist’s Stoop | Repeated and sustained stooping which is an aspect of a persons occupation. (As in the case of former dentists, who, before the invention of height adjustable dental chairs, had to lean forward to extract teeth from patients) See also here |
| Depression Stoop | Many people who don’t pay any attention to detail, and who haven’t studied the cause of postural deformity properly will see someone slumped over, and assume that their postural problems were caused by laziness, a bad habit of sitting and standing, or sadness. However, such factors are probably less than 5% of actual cases. It is also more likely that because of their poor posture they develop health problems which make their lives more difficult, so that the psychological factors are the result of their spinal deformity rather than the cause. |
| Dowager’s hump | Many women over the age of 50 develop an extreme stoop in their upper spine, which is related to fractures of the spine which are partly due to the long term effects of wearing high heel shoes, which alter the balance and shape of the spine, combined with hormonal complications of the menopause, where the reduction in the level of Oestrogen results in osteoporosis, the lose of bone density. The long term effects of poor nutrition, such as the lack of calcium in the diet also contribute to the problem. See slso here and here. |
| Flat foot stoop Also called the shoe stoop | Any abnormality in the shape of the foot will affect the shape of the spine, including the deformity known as flatfoot. The advantage of running barefoot rather than wearing shoes has been described by Harvard professor Daniel Lieberman who has consequently been called the barefoot professor. He says that the primitive tribes people of the past had healthy feet because the front pads of their feet hit the ground first and had a cushioning effect where some of the force was taken by the rotational movement from the front pads to the heel pads, which prevented foot and spinal damage. He further explained that when people wear shoes, the heel of the foot hits the ground first and sends pressure straight up the spine. Furthermore, modern shoes generally have a curve in the mid shoe area which gives artificial support for the arch of the foot so that the relevant muscles don’t get any exercise. Consequently the arch of the foot tends to become weak and collapse causing a condition known as flat foot, as well as the foot pain and other problems associated with it. He adds that modern shoe manufacturers advertise the benefits of sports shoes, but don’t mention the problems they cause. From the TV show called “In Focus”, Channel 44, Adelaide, 11-3-13. See also here and a YouTube video here, and the feet and evolution here. In my own observation, other aspects of shoes cause problems such as the main one – LSE, and the LTF, and EPD etc. See my report on posture and evolution here. |
| Foot Deformity Stoop | Spinal deformity that results from deformities of the feet which alter the bodies centre of gravity, and requires a change in posture to maintain balance. See here Those changes in posture are due to an automatic reflex. The postural problem may also be remedied with shoe inserts or orthopedic shoes designed to counteract the foot deformity. Abnormal foot structures include, Rothbart’s foot, Structural Flat Foot, Peasant Foot, Egyptian Foot, Greek Foot (also known as Morton’s Foot), and Simian Foot. The different types can be seen in the photos here. You can also test your foot-brain connection by sitting at a desk and lifting your right foot off the floor and moving it in clockwise circles. If you then draw the number “6” in the air with your right hand your foot will change direction. For more information see here and here and here and here. See also; this video on foot deformity and posture here See also here |
| Heavy breasts stoop | Large and heavy breasts move a woman’s centre of gravity forwards and can be a cause of stooped posture in some women. |
| Hereditary Stoop | A stoop which is inherited from the parents. Also called Genetic stoop. e.g. Neurofibromatosis (also called Recklinghausen disease) can cause scoliosis (sideways curvature of the spine). See here and here. and Progressive infantile scoliosis video here and webpages here and here |
| Injury Stoop | An injury to the spine or any other part of the skeleton which sets the bones in an abnormal position and alters the bodies centre of gravity. |
| Kit bag Stoop | Carrying a kit bag full of heavy books to and from school every day which results in the gradual development of forward and sideways curvature of the spine. See also here |
| Malnutrition Stoop | Poor diet which results in a loss of muscle tone and body bulk causing the spine to slump forward. |
| Marathon runners posture | The ability to sustain effort depends on oxygen supply to the body, so the size of the lungs will have an influence. I have observed that many marathon runners run in the upright position with a very straight back, or some appear to be inclined slightly backwards, which would have the effect of stretching the chest and slightly increasing the size of the lungs, and the ability to win events. Such a posture would also prevent downward pressure on the chest cavity which would otherwise restrict lung movement. Also any tight belts or bending at the waste would restrict breathing efficiency by preventing full downward movement of the lungs. i.e. by running upright and not bending at the waist the lungs are freely able to move the full distance up and down in the chest. The same advantage would apply to sprinters, where posture, and chest size and shape would determine lung size and capacity. Similar features were also presented on Twitter by Alessio d’Ambrosio on 15-12-13 via a link to a an illustration on pinterest.com where the general recommendation was to run in a slightly forward position, and to lean further forward when running up a hill, but making sure that the runner doesn’t hunch over at the waist. See here. |
| Neck Stoop | Neck stoop can be seen from the side view in a person with a deep chest where the rib cage forms a triangular structure which prevents the spine from collapsing into a C-shape, so it remains straight, but the neck bends sharply forwards. |
| Obesity Stoop | A large and heavy belly which drags the lower spine forwards, where the upper spine stoops to counterbalance the effect. |
| Old Man’s Stoop | Osteoporosis. |
| Optical Stoop | A visual defect in childhood which necessitates repeated and sustained leaning forward to read. |
| Pott’s Stoop | Pott’s disease i.e. tuberculosis of the spine, where an infection of a vertebrae causes the spine to collapse. |
| Pregnancy Stoop | The forward displacement of the abdomen which drags the lower spine forward due to the weight of the pregnant womb, and where the upper spine falls forward to counterbalance the alteration to the centre of gravity. The spinal shape continues to alter as pregnancy advances and the weight of the womb increases, more so if the woman is carrying twins or triplets, and in some cases the changes persist after giving birth. |
| Rice Farmers Stoop | The stooped spine seen in old rice farmers who have spent most of their lives bending forward to tend to their rice crops. See here |
| Rickets | Vitamin D deficiency can produce rickets which softens bones and results in spinal curvature due to the weight of the head and shoulders. |
| Shoulder Binding Stoop | Permanent Strapping around the shoulders which was designed to create a hunchback physique which was fashionable in some seventeent century tribespeople. |
| Sideways Stoop (also called Scoliosis) | Sideways curvature of the spine due to having one leg shorter than the other, or to carrying a heavy kit bag or satchel to school or work, especially during periods of poor nutrition or illness when young and the bones are pliable. The hunchback poet Alexander Pope had one leg shorter than the other and sideways curvature of the spine. See also the videos here and webpages hereditary progressive infantile scoliosis here and here |
| Slouchers Stoop | The tendency to slouch in childhood because the child feels relaxed and comfortable in the slouched position and because the attempt to sit upright causes discomfort and strain on the spinal muscles, especially where there is a mild pre-existing spinal deformity due to other causes. |
| Sports posture | See marathon runners posture. |
| Stiletto Stoop | The wearing of high heel shoes which throw the hips forward, the shoulders backwards, and the head forwards as a counterbalance. (The altered posture throws the woman off balance, and makes her walk with a an awkward gait, which disposes to falls. The long narrow heels also tend to sink in mud, and the narrow surface at the base gives less grip on the ground and disposes to slipping on many surfaces, and tripping over small stones etc.) Women have been wearing high heel shoes for many centuries for reasons of fashion, to make their legs look longer and more attractive. The extra height also gives them the sense of power and the image of authority. See also an item about the change to foot/posture mechanics of rocker shoes here. See more problems such as calluses and corns, which are caused by wearing high heel shoes here. |
| Swimmers posture | Postural compression of the chest due to hunchback posture or lordosis etc., reduces lung capacity in swimmers, so improving posture will improve performance. See here |
| Tall Boy’s Stoop | The rapid growth of the spine during childhood where the tall child also has to customarily stoop forward to read at a small desk, or to talk to smaller children. |
| Women’s Stoop | Women can develop poor posture for a variety of reasons such as by wearing high heel shoes which tilt the lower spine forward and produce a counterbalancing forward stoop in the upper spine. Similarly large breasts can be heavy and drag the upper spine forward and downward. The pregnant woman can develop poor posture as the result of having a large and heavy womb which drags the lower spine forward, and produces a counterbalancing stoop in the upper spine. Also osteoporosis can weaken the strength of bones, and cause the upper spine to fall forward under the weight of the head and shoulders (called Dowagers hump). See also here and here Also see a recent well written account of women’s posture here |
| Vitamin D deficiency stoop | Vitamin D deficiency due to nutritional deficiency or lack of sunlight can cause rickets which weakens the bones and results in curvatures. Calcium deficiency may be another cause. |
| YouTube Videso on the causes of poor posture here and Part 2 here Also see the following article from The Times of India which is a breech of my copyright because it contains a summary of the causes of poor posture which are an exact copy of my theory and website, except for the fact that poor posture is mainly due to biomechanical factors, and not a bad habit. The details and the summary are too exact to be a coincidence. see here and here. |
Poor posture and health – The cause or effect question
The effect on the economy of nations
The main purpose of my 1000 page book, now available as an eBook, was to show the harmful effects of poor posture on health, and how important it is to prevent and treat the problem in children. See here.
I sold many of my books called “The Posture Theory”, to schools, because it is much easier to monitor, prevent and reverse spinal deformities when children are young, and their bones are pliable, than it is to live with, manage, or treat the predictable health problems which will inevitably follow as they reach adulthood, and grow older.
That fact has been known since the 1930’s, and is evident from the life-story of the hunchback poet Alexander Pope here.
It is also evident by a casual look at all of the successful people in industry, academia, and politics. You will notice that their spines are mostly straight, their shoulders are broad, and their chests are deep, so there is no pressure on their abdomen to impair their digestion or stunt their growth, and their is no pressure on their heart and lungs to impede their breathing and stamina, and as Plato said, they are the ones who achieve success in all facets of life.
It is also evident that people with spinal deformity will become more stooped with age, and those with straight spines will develop deeper chests.
Many sensible people accept those facts, and most people who I discuss these things with agree with me, and some take it for granted, as if it is ‘obvious’, but some reject the general idea on the grounds that it is unprovable, and shed doubt on that obvious fact, by arguing that the idea is not ‘scientific’.
They should be held responsible for the fact that many children will continue to grow up and become sickly and miserable adults.
The costs of prevention are trivial compared to the cost of treatment, and loss of manpower to national economies, which is massive.
I recommend that the treasurers of international political parties consider that fact, more than their efforts in saving costs, after the damage to the health and well being of individuals has been done.
There are many children now between the age of four and seven, who have spinal abnormalities. It is quite irresponsible and unethical to do nothing about that, and then argue n thirty years from now that there health problems are there own fault, and are trivial, or due to laziness, fear and mental illness.

The child was described as having a postural defect with Lordosis and “had been sleepless, irritable, and easily exhausted from early infancy”.
My review of a book from the 1930’s
While I was writing my book called The Posture Theory I found an earlier publication from 1930 which discussed the relationship between poor posture and symptoms in children, and the consequences of not treating the postural defect when the child reaches adulthood. It was called “The Nervous Child”, and I reviewed it in the 11th edition of my book on pages 101 and 251, and have given another summary below.
The author of that 1930’s book proposed that nervousness weakened the antigravity muscles of the spine which in turn caused poor posture. However he also made the observation that the exercise programmes provided to army recruits improved their posture which in turn improved their health and temperament. (i.e. that improving their posture made them calmer. Therefore it is poor posture which causes nervousness, and not nervousness which causes poor posture M.B.).
This is another quote from that book . . . “The stance of the nervous child may be described as the opposite of that which the drill sergeant inculcates so vigorously in the recruit”. The curative posture in drill results in improved health and temperament“
Curvature of the upper spine often results in a counterbalancing forward arching of the lower spine which is called lordosis which according to the author of that book, pushes the abdomen forward and causes the chest to recede. This physique tends to produce symptoms of restlessness, irritability and fidgeting, digestive disturbances disturbances, and appendicitis. It is also commonly associated with sore throats, and proneness to colds and tonsillitis
There is also an alteration in the circulation of blood which results in paleness of the skin, alterations in skin temperature in relation to exertion, and a tendency to faintness, breathlessness, palpitations, and motion sickness, which are very commonly encountered with children who have this physique.
He adds . . . “If we encounter these children, so nervous, so excitable, so easily exhausted, with their faulty posture and unstable circulatory reactions and describe them solely with the eye of a cardiologist, we shall describe them as suffering from “cardiovascular asthenia” or the “effort syndrome“. . . and . . . he observes that such children were likely to become sickly and miserable adults and undergo several forms of surgery unless their postural defect was corrected. He suggested that good exercise and
good diet were important, and that children should be provided with properly designed chairs and desks of appropriate height for their bodies, and that the correction of eyesight problems was important so that children did not need to lean forward to read, in which case the constant bending caused the spine to grow stooped.
Reference: The Nervous Child (1930) p.171-189
The relationship between posture and health has numerous aspects which create confusion about which causes which. However it is most likely that various infectious illnesses, especially prolonged illnesses, which impair appetite or result in a loss of weight or a weakening of bones during the growth periods of childhood, are likely to cause the spine to stoop under the weight of the body, and unless recuperation is rapid, the postural alteration may persist.
Thereafter postural pressure on the chest and abdomen would dispose to numerous health problems. However as long as the child remains active they may be free of most symptoms, but if their lifestyle remains predominantly sedentary, the constant effects of stooped posture may then bring about a variety of ailments in adulthood. M.B.
Popular MYTHS about the cause of poor posture
it is popular to believe that slouching is due to laziness, or because the person doesn’t want to sit up straight.

However, the major factor which determines the way a person sits or stands is the shape of their spinal bones. That shape can be determined by an injury which occurs in a few seconds when the person is young, or by poor nutrition or disease which weakens their bones and causes the change in a few weeks or months. Needless to say that if the postural problems are not corrected when the child is young, then the change in shape will become permanent as the bones harden in adulthood. It is impossible to straighten adult bones just by sitting up straight.
Other cause or effect questions
it is also popular to believe that a child develops poor posture as the result of a bad habit, but spinal deformities have physical causes and standing in a particular way is much more likely to be a counterbalancing response than a habit.
The other popular misconception is that sadness causes poor posture, however, it is much more likely that physical factors result in spinal deformity, which in turn causes health problems, which then causes misery as a consequence. Also poor posture can affect the circulation of blood adversely to cause lethargy, and impede blood flow to the brain and have an effect on such things as the ability to concentrate and tiredness etc..
There has also been the suggestion that poor posture is due to stress and muscle tension, but in order to slouch the spinal muscles need to relax and stretch, and, for example, many people slouch in a lounge chair when they are relaxing as they watch sport on television.
It is important to develop effective methods of preventing postural problems, but that is more a matter of education than anything else.
A collection of diagrams from the 300 in The Posture Theory
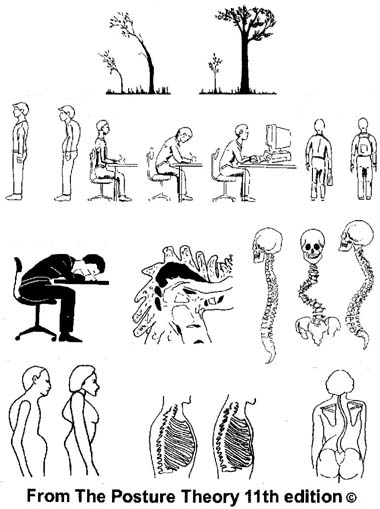
Top diagram | Alexander Pope wrote “Just as the twig is bent the trees inclined. |
| Row two left | Good and bad posture. |
| Row two centre | Good posture at a desk, and curving forward from the hips, and improperly bending the neck. |
| Row two right | Sideways curvature of the spine can be due to carrying heavy books to school in a satchel held in one arm, compared with a knapsack where the weight is evenly distributed to both sides of the spine. The knapsack should be put on properly, and the books not too heavy, or they can cause a forward stoop in the upper spine, or a forward arch in the lower spine. See also here. |
| Row three left | Extremely bad reading posture due to poor eyesight. See also here. |
| Row three centre | Hunchback posture due to tuberculosis of the spine. |
| Row three right | Good posture, sideways curvature, and stooped curve of the spine. |
| Bottom row left | Stooped posture with a flat chest, compared with a deep chest. |
| Bottom row centre | Normal ribs compared to compressed and permanently flattened ribs due to poor posture. |
| Bottom row right | The abnormal angle of the shoulder blades due to sideways curvature of the spine. |
An explanation for the illustrations
When a child is young their bones are soft and pliable. like the trunk of a young tree, especially if they have poor diet, or a long viral illness that affects their appetite, so a variety of factors can change the shape of their spine. For example, sleeping for eight hours every night in a spring mesh bed that sags in the middle, or repeatedly leaning forward to read due to poor eyesight, or being tall and having to bend their neck to talk to smaller children may gradually affect the shape of their spine. If the child carries heavy books to school in a satchel held in one arm he is likely to gradually develop sideways curvature of the spine, depending on the weight of the books, and the strength and physique of the child, and the distance traveled each day, and of course, on his nutrition. That problem can be prevented by carrying books to school in knapsacks on their backs where the weight is distributed evenly across each side of the spine, but they need to be put on properly, and not be overly heavy or the student may develop forward curvature of the upper spine, or a forward arch in the lower spine.
As the child grows the bones will curve, and the ligaments and muscles of the back will stretch accordingly, and then the bones will gradually harden by early adulthood . As you can appreciate, it is much more difficult to bend adult bones back to their original shape, and is comparable to trying to straighten a bend in the trunk of a fully grown tree.
However, surgery is sometimes performed in extreme cases of deformity, but the problem can be managed by developing a good understanding of anatomy, and by using methods of sitting and standing which restore effortless balance. The Alexander technique and Yoga provide some insight into those methods. However, as they say, prevention is better than cure.
If poor posture is not prevented or properly managed it can lead to many other health problems where the most commonly known ones are backaches, inefficient breathing, and lethargy – for example they are often referred to as ‘slouches’ – who haven’t got enough energy to do anything.
Some of the effects of poor posture or other types of compression

Culturally induced deformities: The ancient Greeks wore loose garments, and were very healthy compared to other cultures who deformed their bodies by using such things as shoulder binding straps to deliberately produce the hunchback appearance.
Seventeenth century women believed that it was attractive to have a long thin neck and sloping shoulders, so they wore binding straps to achieve that permanent appearance.
The Flat Head Indians of North America strapped boards to the top of the heads of their babies when their skulls were pliable, so that they grew up to be permanently flat in adulthood. They were known to neighbouring tribes to be somewhat dull, probably because the deformity of their skulls affected their brain function.
Education in the history of fashion and health can prevent those problems from occurring to future generations of children.

| Left | A cartoon showing the effects of high heel shoes on the spine. See also here. |
| Centre | A normal foot compared to a foot permanently deformed by wearing pointed toe shoes. See also here |
| Right | Sideways curvature of the spine (scoliosis) caused by having one leg shorter than the other. A cause of back pain which can be relieved by inserts or raised soles and heels on one shoe. |
 |
|
The Posture Theory and Chest Shape ©

The lower diagram, and the geometric comparisons have been adapted from it. M.B.
If an individual has good nutrition and good health when they are young they are likely to develop a natural spine and chest shape.
The natural shape of the spine, when viewed from the side, is upright with a slight S-shaped curve, and the breast bone is slightly inclined forwards. The breathing muscle or diaphragm forms the base of the chest, and is dome shaped when the person breathes out, and flattened when they breath in.
The overall shape of the chest is therefore triangular, and moves to a somewhat pyramid form if they lean forward or stoop their head, and the overall arrangement is structurally stable.
By contrast, if the individual has illnesses like rickets or prolonged viral infections which weaken their bones and muscles when they are infants, the spine is likely to bend forward under the weight of their head and shoulders, and as the spine forms a C-shaped curve, the lower spine pushes the lower abdomen forward into a pot bellied appearance. That physical shape forms a crease across the front of the upper abdomen and the lower tip of the breast bone tends to be caught in it and pushed backwards each time the child leans forward.
When the breastbone is flattened in that manner, and runs parallel to the spine, it has the shape of a column, more like the leaning tower of Pisa.
The net result is that the child with a triangular shaped chest will tend to push the breastbone forward as they grow, so they will naturally develop a deep chest with a lot of room for their heart and lungs and stomach below, which allows for good digestion, good breathing, and plenty of energy, which, in turn, gives them a competitive advantage in the pursuits of life in sport and business.
However, the child with the stooped spine will have a flat chest, that tends to incline backwards, and doesn’t support it, so the spine will become more stooped as they grow. That will tend to limit the room available for the heart, lungs, and stomach, and therefore result in impaired digestion, respiration, and energy levels.
The importance of this concept to parents, educators, health professionals, and public health officials is that the effects of such illnesses on the physique of children needs to be identified as quickly as possible, and then good nutrition, and natural activities and exercises encouraged as soon as possible after recovering, so that permanent and progressive problems can be prevented.
The idea that a combination of posture and chest shape is the cause of multiple symptoms is unique to The Posture Theory.
The Posture Theory and the aspect of Evolution © M.A.Banfield
Many ideas appear to be simple but it takes thousands of years before one man thinks of it, and then it becomes obvious. This is what one of Charles Darwins most famous advocates, Thomas Huxley, wrote about his theory about the origin of species. . .
“How extremely stupid not to have thought of that!” See here
According to Newton’s third law of motion action and reaction are equal and opposite.
However, I have noted the axiom, that in evolution, reaction is slightly greater than action. © M.B.
(re: As time goes by, the difference from the original becomes progressively greater).
Charles Darwin had a writing platform bulit onto the arms of his arm chair, and a tall music stand can be seen in a photo of his home. See my report here
According to Darwin the average person knows no more about the insides of the human body than they know about the inside of a ship.

When I first wrote the posture theory I was describing how poor posture places the head and shoulders forward of the bodies centre of gravity to produce strain on the spine and compression of the chest and abdomen which would cause chest pains, fatigue and indigestion.
I also considered the possibility that the harmful effects of poor posture on health may have contributed to the evolution from monkeys with a stooped spine, to man with an upright posture.
The apes, for example, have long strong arms which enable them to swing through trees with ease, but when they move down to the ground they walk with their spine straight, but bent forward from the hips in a posture that is halfway between standing upright and walking on all fours. However, they tend to support the weight of their head and shoulders by placing their hands on the ground.
By contrast humans have gone in the opposite direction and walk upright with the weight of their head and shoulders balanced effortlessly on top, which would make movement on the ground much easier.
Another factor would be the shape of the chest. For example, when viewed from the side a deep chest has a rib cage which takes on a roughly triangular shape which would tend to act like a framework that prevents the spine from bending in the middle. By contrast the flat chest would have a virticle shape, and the torso would tend to buckle in the middle and press backwards into the body and bring the upper spine forward and over into a stoop to make health problems more likely.
Hence those humans who had good posture would tend to have good digestion and stamina and thrive more so than those with poor posture so that eventually most humans would have an upright posture.
The diagram above shows, from left to right, the posture of a Gibbon, Orangutan, Chimpanzee, Gorilla, and Man.
The next two are from the first few pages of my 1000 page book called “The Posture Theory (11th edition)”, and show a man leaning forward to read, and placing his elbow on the bench and his hand on his jaw to support his upper body and thereby reduce the strain on his spine. The final diagram shows the man standing at a desk and typing on a keyboard which is placed at waist height, and looking at the diagram on the screen which is positioned at eye height so that there isn’t any need to bend forward. It is an effective way of relieving and preventing several health problems.
The first five illustrations are from a book called “Anthropology: An Introduction To The Study Of Man And Civilisation” (1881) p.39 by Sir Edward Burnett Tylor, which was previously from “Man’s Place in Nature” (1863) by Thomas Henry Huxley, where the gibbon was represented as twice normal size. That part of the diagram was originally drawn by Mr. Waterhouse Hawkins from specimens in the Museum of the Royal College of Surgeons.
I used that diagram on page 150 in the eleventh and final edition of my book in October 2000. The next two diagrams have been adapted by me from an illustration in a book called De humani corporis fabrica by Andreas Vesalius in 1543. The first adaption was used as the cover for the 4th edition of my book in November 1994, and the second was added later, and both have been featured on the first two pages since the 10th edition of August 1999.
This aspect of The Posture Theory is a suggested extension of Charles Darwin’s Theory of Evolution. © M.A.Banfield October 2000 with modifications on 16th October 2010.
I started reading some biographies of Charles Darwin about fifteen or more years after I wrote The Posture Theory, and noticed that he had similar health problems to the ones I had been studying, I also noticed that he sat in an arm chair which had a tailor made writing platform set into it. Photos of one of his rooms in later life showed a tall music stand for reading sheet music from the standing position.
Charles Darwin, like most people who develop new ideas which bring old ones into question, was criticised and subjected to ridicule and mockery. In fact, if he did not have other intelligent supporters who were prepared to champion his theory then his ideas would now be just an obscure nineteenth century novelty, and many unscrupulous writers would have plagiarised everything he wrote to claim the ideas for their own financial or social benefit. M.A.Banfield.
The following quote comes from another website . . . “Your Mother Was Right – Posture is Important! . . . When doctors or therapists look at someone’s posture they generally first look at the alignment of the weight bearing joints in standing. ideally from a back view the spine should have no lateral curvature and the legs should be symmetrical without undue angulation at the knees or ankles. From a side view the spine should form a smoothe S-shaped curve, bisected by an imaginary plumb line dropped from the apex of the head through the centre of gravity of the body. This same plumb line should pass through the tip of the shoulder, the center of the hip joint and ankle joint and slightly behind the knee joint. With this ideal alignment the body weight is balanced over the spine and lower extremity joints requiring minimum muscular effort. This alignment also evenly distributes pressure on the intervertebral discs and avoids excessive stress on the ligaments . . . The sitting position is where most of us get into trouble with poor postural habits. This is especially true when driving or using a computer. As we focus on the activity in front of us we tend to protrude the head and neck forward. Because the body follows the head, the thoracic and lumbar spine tends to round forward as well.” (the author is FRANK J. D’AMBROSIO, PT – apparantly a website essay – date unknown. See more information here
I invented the idea of standing at a desk to improve posture in 1994

I wrote The Posture Theory in 1980.
The photo above shows my computer layout.
In 1994 I added a plat
form to the top of the desk.
In 1998 I learned to type and added another platform on top of the first, and then added a keyboard tray to bring the computer screen higher.
The keyboard is at elbow height, and the screen just below eye height.
I have been standing to type ever since.
I started trying to determine the cause of my health problems in 1975, and soon concluded that sitting as a desk and repeatedly leaning forward to read and write was somehow associated with inducing and aggravating my abdominal pain. In fact, that idea is part of The Posture Theory of 1980.
During that period I spent most of my time laying on my back and staring at the ceiling and trying to think how to solve those problems, and would spend as little time as possible writing my conclusions down on paper to send off for publication. As a general guide I would spend two weeks thinking which didn’t cause any pain at all, and then several hours or more writing, often in stops and starts, which was followed by two weeks recovering from the abdominal pain that was caused by sitting for that short time at the desk.
I also tried to improve my posture while in the sitting position to see if it would prevent the pain but it was not very effective. In fact, if I leaned forward I would gradually accrue pain, and if I sat up too straight I could feel a stretching pain in my upper abdomen, so I found it too difficult to find a medium position which was consistently comfortable.
Fourteen years later I decided to add a small platform on top of my desk to raise the height of my writing paper to see if it would consistently improve the upright position of my spine and reduce the postural pressure on my stomach, and the pain. It did, so I published an illustration of a skeleton standing at a high desk as the cover diagram on the fourth edition of my book in March 1995. Sometime later I started to learn how to type, and then use a computer, and in about 1998, I decided to raise the screen to eye height for the same reason. That change resulted in a major reduction in the severity and duration of that symptom. Naturally, the volume of writing that I was capable of after that year increased. The diagram of a skeleton standing at a desk with the computer screen at eye height was the first full page illustration in the tenth edition of my book which was published in August 1999. The eleventh edition was published with those illustrations in October 2000. I used the same diagram on the cover when I published the 12th edition as an eBook recently, in July 2012. It is available through here. See my YouTube video on how I developed the original theory here.
I used diagrams of what was happening to the skeleton and the internal organs to show what other people could not see because it is covered by a layer of skin.
When I changed my posture in that manner I predicted that the focus of my body weight would change and that it might cause other problems. I did notice, after several years, that I was getting more leg cramps, foot aches (which I had never had before), and some minor problems with haemorrhoids, and I found them reasonably easy to manage by reducing the time spent standing at the computer, having regular breaks, and walking about. Also the change did not completely remove my original symptoms, but it did reduce their number and severity considerably. People with normally shaped spines, and effortlessly balanced body weight, would probably not have any health problems, and would not need to change from the sitting to standing posture. Similarly some people might benefit from other methods. It depends on the individuals physique.
I also knew that sooner or later some people would recognise the health and financial value of my ideas in preventing and treating disease and would start using them.
Imitation is the best form of flattery
I invented the method of standing up as a way of preventing health problems caused by sitting at a desk as early as 1994, and modified the method to make it much more effective in 1998. See a summary of my theory here and the ebook version of my book here.
Since then I have seen TV shows which report that other people have copied that idea, or drawn a similar conclusion. A more recent website with a similar idea can be seen here.
See also a report published by another author named Jon L. Gelman in 2012 about the use of sitting/standing variations as a means of preventing back pains and improving circulation, energy levels, blood flow to the brain, concentration, and sleep patterns, here.
I read that page on Monday 17th December 2012 and sent the author an email informing him that he may have inadvertently breeched my copyright as they were virtually an exact copy of the details in my theory. I also asked him to comment on my report, and when I checked it the next morning it had the words . . . “Sorry, the page you were looking for in this blog does not exist” (end of quote) The advantage of him deleting that page is that he is no longer breeching my copyright, but the disadvantage to me is that some the evidence of the accuracy, and merit of my ideas is gone, as well as the fact that many other researchers at the highest levels recognise their importance and usefulness and are scientifically proving them, but have not known or acknowledged me as the source. |
This is a quote from that article . . .
“Over the past year, NIOSH and its Total Worker Health Program have been traveling the country sharing the evidence and benefits of comprehensively integrating health protection with health promotion, including workplace programs that encourage physical activity, weight loss and stress management. Recently, we launched an internal NIOSH pilot program to explore the use of sit and stand work stations as part of a workplace health and wellbeing initiative to reduce sedentary work in our workplace.
The pilot program was inspired by emerging research on the impact of sedentary work (Van der Ploe, Chey, et al, 2012) on employee health and by new employer initiatives that aim to decrease sedentary work, such as VHA’s Wellness Program highlighted in a recent NIOSH Science Blog post. A sit-stand workstation allows the user to intermittently sit or stand while working on the computer, participating in a conference call, or performing other work. The customizable workstation allows users to easily transition between a seated and standing work position multiple times throughout the day” (end of quote) That quote can also be seen in the CDC Centers for Disease Control and Prevention website here.
This is some more quotes from another website called ISHV . . .
“Walking workstations were placed in departments where several employees could share them (see photo). These devices, essentially treadmills with desks, computers and phones attached, allow staff to walk at a slow pace (1-2 miles per hour) and work at the same time . . . and . . . Employees received accelerometers to discourage sitting still. Unlike pedometers, accelerometers measure vertical acceleration and some vibrate when the user has been still for a period of time . . . Preliminary evaluations show that these efforts are paying off in a trimmer, healthier VHA workforce . . . Based on the success of the program they worked with a multidisciplinary task force to develop The Employee Health Promotion and Disease Prevention Guidebook. The aim of this guidebook is to provide health care professionals with information and references appropriate for establishing and expanding programs at individual facilities . . . We would like to hear from you. Share with us your successes in improving the health of your workforce. What are some of your challenges?(end of quotes) See here
As the authors wish to hear from readers I would like to inform them that I am the person who developed those ideas and principles many years ago, and as such I am entitled to be recognised for that.
Jon L. Gelman’s qualifications Jon L Gelman is Managing Attorney – Education – John Marshall Law School, Chicago, Illinois, 1971 Doctor of Jurisprudence – Rutgers The State University of New Jersey, New Brunswick, New Jersey, June, 1967 B.A., Bachelor of Arts Major: Political Science. He has published several books and has received many honors and awards, and is a member of many professional law associations. His profile can be seen here This is a quote from the Jon L.Gelman website as of 10:18 A.M. 15th November 2012 . . . “Providing legal service with a social conscience . . . The law firm of Jon L Gelman has been listed in the 2013 edition of America’s Best Law Firms Rankings of U.S. News Media and Best Lawyers.. . . Jon L. Gelman stated, “It is indeed an honor to once again be named to this list. For over 4 decades it has been our privilege to represent and assist injured workers and their families.” See here |
Does the Adelaide TV show called “Today Tonight” deserve to be trusted
I spent 23 years trying to develop a way of relieving or preventing my own abdominal pain which occurred intermittently, and varied from annoying aches, to severe, completely disabling, and relentless pain which lasted for several months at a time. When I succeeded and described my method I did it to help other people to prevent or relieve similar problems, and not so that copyright thieves could read about it in a few minutes, and steal the idea, and claim it to be their own, or find out about it, and write or discuss it without mentioning my name. See more here.
Some friends of mine know the truth
Some friends of mine have visited my home and seen my computer room where I stand in front of computers, and they have asked me why they are all on top of benches, and why I stand in front of them instead of sitting in a chair.
I have explained that I started experimenting with writing or typing on platforms of various heights since 1994, and invented the standing computer position in 1998, and explained why.
I then showed them my published essays from the 1970’s, and the eleven editions of my books which were published from 1994 to 2000.
I also showed them the first and main diagram of the 11th edition which shows a man standing at a computer, and looking at a computer screen with the picture of a man sitting at a desk, and all of the angles and health problems listed.
They all know that I am the inventor of that method, and that I can obviously prove it.
They have asked me why Today Tonight has interviewed University professor John Coveney, instead of me.
I have told them that I have contacted the TV producers by email and phone to let them know that I am available for an interview, but they haven’t replied.
Approximate Time frame and empirical science compared to conventional science
I first experienced obvious abdominal pain in about 1972 but none of the medications prescribed then or since had anything but temporary effect. I began studying that problem myself in 1975, and wrote an essay about it called “Riddle me riddle me re: from my bellyache I flee” which was published in the Australasian Nurses Journal in April 1981. The pain was intermittent and a few years later was so severe that I asked a surgeon to cut my abdomen open and see if he could find a cause. He did the operation but couldn’t find anything. I was diagnosed with cancer in 1994, and started writing a small book, but still had pain after a few minutes of writing, so I only wrote small sentences or paragraphs at a time. In the next few years I tried to prevent the pain by adding a six inch high bench to the top of my desk so that I would be less likely to bend forward and compress my abdomen when I wrote. I later added another six inch high bench on top of the first. I also tried to write on a high platform while standing up, but it only resulted in a small amount of relief. I then experimented by reading or writing with my papers on angled platforms, and later learned to type, and then how to use a computer. Over a period of months or years I experimented with placing the computer screen on platforms until it was higher, and then higher again, until ultimately the screen was at approximately eye height, and the keyboard was at elbow height, when for the first time in 23 years I could write (by typing) without getting abdominal pain.
International researchers can steal that method in a few minutes, and claim to have thought of it themselves, but as you can see they were never going to develop that idea in their laboratories while looking at blood under microscopes, or anatomy with x-rays.
The method which I invented in 1998 is now being taught by “Adelaide’s standing professor” to university students in 2013
The reporters of the Adelaide TV show called “Today Tonight”, including Paul Makin, and others, are fully aware of my CFS/Exercise research from 1982, and since, but they refuse to interview me on that subject, and have therefore been giving local and international researchers the opportunity of stealing my intellectual property, and taking the credit for it (including Simon Wessely and Peter White of London via their PACE trials here).
Recently they did a segment called The standing professor which essentially LABELS him as the inventor of my method of standing at the computer to type instead of sitting at a desk. See here. The label will leave that impression on the public mind regardless of whether or not they actually said it in the interview. Therefore I consider their actions to be unethical and irresponsible, and rang the TV station to seek an interview to make the public aware that I was the inventor, and not Professor Coveney, or some unnamed mystery person from the U.S. I was diplomatically fobbed off by the statement . . . ‘we will look into the possibility of discussing my invention in the next six months“.
I suppose they can childishly react out of spite, and use my comments here as another excuse for not telling the public the truth about who has developed such ideas, but they have left me no other choice. I want the public to know that whether or not they choose to respond in an ethical way or not, is up to them, but I don’t want them to have the ability to fob me off like that interminably, in secret, in order to evade their duty to be honest, open, and accountable.
I studied that problem for 23 years where I often experience up to 3 months of severe abdominal pain, where medication and all other forms of treatment were all but useless, before I developed that method, However, people with that or any other posture related problem who copies me can gain those benefits in a few minutes by being told about it. Intellectual property thieves can also copy me within a few minutes without having to endure 23 years of pain.
My comments on their report on Adelaide’s Standing Professor can be seen below.
Adelaide’s Standing Professor
John Coveney and My intellectual property rights Since writing the report below I have phoned John Coveney in his office at Flinders University and informed him that I am the inventor and developer of the theory and method for the standing computer position, and I explained that it was the first diagram in the 10th edition of my book called The Posture Theory which was published in Adelaide in August 1999, and that it is the cover diagram for my ebook of 2012, which is the 12th edition. He listened politely and agreeably and did not dispute the evidence and proof that I provided. I therefore have no objection to him using my method for the benefit of his own health, or for discussing, or researching it to confirm it’s value in the peer reviewed sense, or for teaching about it in international health conferences. However I require him to refer to it as Banfield’s Standing Computer Posture, to avoid any misunderstanding about who developed the idea. I assume that he will, for ethical and professional integrity reasons, not give the impression that it is his own idea, or that it is somebody else’s other than mine, and that he will respect the amount of research and experimentation that went into it, and acknowledge that it is subject to my copyright, and honor my intellectual property rights, and that anyone else who uses it will do the same |
I spent 23 years developong and refining my theories on posture and health before concluding that many of them could be prevented or relieved by standing in front of a computer to read or type, instead of sitting at a desk. Fifteen years have gone by since then.
Professor John Coveney is reported to have spent the most recent ten years observing the increased risk to life of the sedentary posture.
As I have never met him, and he appears to be unaware of me or my theory, he is essentially presenting an independent, unbiased, and peer reviewed verification of my prevention and treatment method.
*********
On Adelaide’s channel 7 TV show “Today tonight” on 10-9-13, host Rosanna Mangiarelli presented a segment in which she referred to professor John Coveney of Flinders University as “Adelaide’s standing professor“. He claims to have been standing at a desk himself to treat his own health for ten years, and has been observing the increased risk to life during that period (ie. since 2003, which means that he started 5 years after I invented and published the idea in 1998. See an ebook version of my book here – Note that the cover has a picture of a skeleton standing in front of a computer, and looking at a man on the screen who is sitting and leaning toward a desk with all of the health problems listed).
Several other authorities in the field described sitting at a desk all day, and then again at night, when watching TV, as harmful to health in “many” ways, and that it wasn’t just because of the lack of exercise, but because of the sitting position (my theory). They also gave the impression that such ideas began in America, and that an American company was selling stand up desks with treadmills for about $1000 each and are now distributing them in Australia. See here.
I cannot be sure if professor Coveney has or hasn’t heard of me, or genuinely believes that the method started as an original idea in America.
Nevertheless the fact that someone is using my method for the benefit of his own healte, and is teaching others of it’s importance, is an academic peer reviewed proof and endorsement of the high scientific standard and value to society of my ideas.
(Note that I wrote my books called The Posture Theory, and sold them to school and public libraries throughout Australia to teach parents and teachers and students how to develop healthy bodies. I also wrote them to show that health problems amongst sedentary workers were due to physical factors, and not psychological factors or stress as had been believed before).
This is John Coveney’s qualifications
“Doctor of Philosophy 1996 (Murdoch University,Perth, Western Australia); Master of Health Personnel Education 1985 (University of New South Wales, Sydney, Australia); BSc (Hons) Nutrition 1977 (University of Surrey, Guildford, UK); UK State registration in Dietetics 1977 (University of Surrey, Guildford, UK); Accredited Practising Dietitian (Dietitians Association of Australia . . .
Honours, awards and grants awarded fellowship of the Public Health Association of Australia in 2012 . . . Key responsibilities
Professor Discipline of Public Health Associate Dean, Prevention, Promotion and Primary Health Care cluster, School of Medicine . . . Co-Director, Physical Activity and Nutrition Observatory: Research and Monitoring Alliance (PANORAMA) . . . =Teaching interests: teach students on the following programmes: Master of Public Health, Doctor of Public Health, Master of Health and International Developments. Bachelor of Nutrition and Dietetics and Master of Nutrition and Dietetics.” (end of quote here).
It is another one of many examples of researchers who use my ideas without knowing that I produced them, or who copy them to gain the credit,
How abdominal pain affected my writing style
(The item below was written long before I found that the stand at desk methods were being referred to as “new” by other authors in December 2012)
The basic problem that I had when reading or writing was that I would sit at a desk, and begin to read or write, and within a few minutes would start to get an ache in my upper abdomen. I also noticed that the longer I wrote the worse it got, and the longer it persisted after I stopped.
Consequently, the process of solving that problem began with me writing one essay every six weeks, and later I was writing 100 word letters to newspapers each week, and then I published a one-word-a-day calendar for a public speakers organisation. Some time later I spent seven years writing a thousand page book which is completely different than any other. It is not a continuing storyline of chapters, but is a series of sentences, paragraphs, quotes, diagrams, and occasional essays which were each written in a few minutes or hours, and have been put into sections that contains similar information about particular symptoms. In order to make the relevant information available to readers I linked the individual items to a table of contents at the start and an index at the end.
My capacity to write has continued to increase with refinements to my methods, but the fact remains that it still causes me some health problems, and it is still a process of stops and starts.
Of course, the conclusions that I have drawn have an element of controversy because the previous ideas in general literature were that the symptoms were imaginary, or ‘all in the mind’, or psychosomatic, and there are some people who obviously resent the idea that I am producing different explanations.
Hence, rather than acknowledging the extreme pain I have been through, some individuals comment on the “peculiar” nature of my writing style, and one of Wikipedia’s anonymous editors who knows how much pain it would have taken to do all that, made an insolent and snide remark to give another editor the false impression that I was telling lies. That editor wrote these words . . .
“Based on his prolific output, I think it would be fair to say that writing is not especially difficult for him, but perhaps we should not assume that it is trivial. WhatamIdoing” 17:28, 5 August 2008. (end of quote). See here.
That individual, who could do up to 300 edits per day in comfort, also deliberately wrote great volumes of criticism to get me blocked and banned, in the full knowledge that I would not be able to keep up the pace. e.g. See here, and here and here.
Another possible cause of abdominal pain – Optical problems
My main conclusion was that the abdominal pain was due to the compression of my abdomen each time I leaned forward to read or write. It relates to other observations that the same pain could occur when I leaned toward benches of any sort, and occasionally when I leaned forward to tie up my shoelaces etc. However, I also considered many other possibilities including the fact that it may be due to a visual problem which related to measles infecting my eyes at the age of five.
See also a link provided by Tom Kindlon on Twitter on 2-11-13 to a research paper in the British Journal of Opthalmology, by Claire V Huthcinson et al, called “Vision-related symptoms as a clinical feature of chronic fatigue syndrome/myalgic encephalomyelitis? Evidence from the DePaul Symptom Questionnaire” here.
The impact of my theories and methods has gone viral world wide
I have recently became aware, that since I invented the theory and benefits of the standing computer posture in 1998, that it is not just one person or organisation that has been “using”, “copying”, or “stealing” my ideas, with many of them claiming them to be their own. Other people may be using, or talking about my ideas without knowing where they came from, but see one of many websites here, and a couple of many You tube videos on the “standing computer stations” below, which are available today, as of 20-10-13.
I must surely be the world’s most influential researcher of the 20th and early 21st centuries, and my ideas have been confirmed and verified by more anecdotal and peer-reviewed studies than any 10 other top theories put together.
The Posture at work: A unique exhibition at the Berlin Museum

Since producing the essays above, I have found a comment on twitter by Retronaut with a link to his webpage about the right and wrong posture at work. It has this quote . . .
“The knowledge that correct posture plays an important role in work has led to a unique exhibition in worker protection at the Berlin Museum. As the German economy becomes more rationalized, it’s important to adjust posture at work to meet modern demands.”
The following photo is from the 1930’s. See here.
ABC TV show “Catalyst” is now telling their viewers my idea without mentioning my name
In 1975 the only suggestion about sedentary workers health problems was that they must be caused by the psychological stress of mathematical calculations, boredom, or the responsibility stress in managers.
However, I developed the posture theory to explain an entirely physical cause for those problems and have had to put up with a lot of ignorant skeptics and critics ever since, who keep arguing that the illnesses are mental or not physical.
Nevertheless, as you can see many of the worlds top researchers and health authorities are using and teaching that method, and some of them have stolen the ideas from me, and others are not aware that I was the producer of those ideas.
I have also contacted radio, TV, and newspapers to report on my ideas but they haven’t.
Recently, on 19-10-13, the ABC TV show Catalyst did a report on the health problems of sedentary workers, and how big business organisers and employers are designing their offices so that workers spend less time sitting, and more time standing and walking about.
It was sitting at a desk that ruined my health, and I was the first person in several thousand years to discover that fact, which is why I wrote The Posture Theory. If I had not written that idea, and later, the standing computer position, then the problems would still be a mystery because no-one else would have found out. It took me 5 years to develop, not 5 seconds to read, or 5 minutes to watch on TV.
I suppose I will write an email about this to Catalyst, but perhaps the public will DEMAND that they interview me.
There are too many people stealing, or later using my ideas, that I simply can’t keep up with all that thievery.
I am only one human being, not the total police staff of SCOTLAND YARD.
Adelaide TV show called “Today Tonight” using my allergy treatment
Most people, rich or poor, ordinary or famous, go to doctors or watch TV to get “instant” cures for their diseases, or raise millions of dollars, or even spend their life savings to fund research, and give awards to those who get results.
I have previously contacted the producer of Today tonight regarding the fact that my research into chronic fatigue and exercise, between 1975 and 1983, which proved a concept, preceded the interest of Simon Wessely, who started in 1987. He has since been awarded the John Maddox Prize for “courage in science“? in December 2012, for his research into that controversial aspect, where he is reported as developing “new” methods? of treatment such as graded exercise therapy, pacing, and CBT, and a Knighthood, for similar reasons. I didn’t expect the TV show to discuss the issue of him copying me, but I did ask them to interview me to give me the opportunity to tell the public of South Australia about my research in 1982, but they sent replies requiring more evidence etc. Half a dozen newspaper items about that project were sent, together with scans of my research paper here, but they have not responded.
More recently they have interviewed John Coveney and described him as “Adelaide’s standing professor“, with his comment that he has been using and evaluating the method for the benefit of his own health for 10 years, and that he discusses it with his colleagues and students.
I advised the Today Tonight TV show that I developed that method in 1998 to successfully relieve 23 years of severe recurring abdominal pain which affected me when sitting at a desk and leaning forward to read and write, and that I used an illustration of the standing posture in the 10th edition of my book, and that more recently as the cover diagram of the 12th edition which was published as an ebook, and I gave them a link to it here. Again, they have not interviewed me.
Last night they did a segment about allergies, in particular hay fever, in which they interviewed a doctor who said, amongst other things, that grass, grain, and tree pollens were responsible, and that they can get into pillow slips if the are put on the outside clothes line to dry after being washed.
I will be sending that TV show evidence that I invented a method to treat an allergic reaction to pollens, namely severe itching, in 1980. It took me many years to deduce that cause because the pollens were invisible, and I had to determine what was happening by logical evaluation. Ultimately I sovled the problem by hanging my clothes etc indoors which reduced the severity of the problem by 50%. I then had a series of desensitisation injections from a dermatologist which finally stopped the allergy, and many years later I found that I could hang my clothes on outside lines again without problems.
The evidence that I invented that method can be seen in an essay called “What caused the itch“, which was published in a N.S.W. nurses journal called “The Lamp” in their June 1980 edition pages 33-34.
That idea would have become known to thousands of nurses and doctors throughout Australia and overseas, and have entered the general discussions and knowledge.
When I was discussing my own problems with itching I met other people or their friends who would tell me that the itching was so bad that the were often contemplating suicide, and some did, so my method would have been extremely valuable to them.
The doctor on Today Tonight might not have known about me, or that research, but he would have gained it from the general literature, and it was my research findings.
I will be writing again to the producers of Today Tonight TV show, and asking them again, to show some respect and do me the courtesy of interviewing me, and letting me tell the South Australian public that I produced those ideas before the other people concerned.
In the meantime I want the readers of my website to check the facts, and decide for themselves.
 |  |
It often took me many years to develop effective ways of treating symptoms or diseases, and then to publish them to help millions of other patients, as you can see from my essay about itching, However, it only takes a few minutes to steal those ideas and ignore the person who produced them and take them for granted as if they have no real value. Nevertheless, without those methods the suffering, distress, and even suicides would still be occurring. See one of my reports on copyright thieves here.
Dr. Bruce Wauchope and my exercise methods for treating CFS
![]()
![]()
Newspaper article reporting the success of my research project in 1982-3
Introduction
I have discussed my research and support groups between 1975 and 1984 elsewhere. e.g. here and here, however, a few years after I started and stopped a group, I saw an article about a new one and attended. The woman in charge was discussing the possible viral cause, which I didn’t agree with at that time but I thought that she was doing an excellent job of helping people so I left the meeting. About a decade went by when I saw another article, and attended a meeting run by Peter Cahalan, who I later learned had a daughter with CFS. It was an excellent meeting, so I suppose I attended on average one every couple of years for another decade. There were even occasions when I mentioned my ideas of a postural cause which seemed to be resented so I rarely mentioned them, and one day I realised that there must be several different causes and types of CFS.
I suppose it was a few years ago no that I attended a meeting an noticed that Peter Cahalan wasn’t there any more and it appeared to be run by a committee of patients, who, naturally, because of their fatigue, would find that difficult, but do-able, and in my opinion deserved respect for that, but I didn’t want to be involved so I just attended and watched, and occasionally made comments.
Kate Fenewick
In the past two years I have offered to give them talks on such things as my exercise research from 1982, but they did not reply so i didn’t pursue the matter, I was therefore curious when I found out about a meeting by Kate Fenewick who was going to give a talk on CFS and exercise.
I arrived at the venue and there were probably 25-30 people there, and then Kate was introduced and began her talk.
Almost every word she spoke was an exact copy of my ideas and methods, and as the audience asked questions she gave exactly the same answers as I have suggested, and the people there were very interested, agreeable, and grateful. She did however refer to her own problem of having to manage the ‘crashes’ which she described, so she is obviously not aware of how I prevent those.
She also works three days a week and earns money by running sessions in a swimming centre to help CFS patients learn the exercise methods.
I have no objection to here doing that, but I do object to her claim that she developed those methods herself, because she didn’t. She has copied me. She also gave out pamphlets which gave helpful information, but when I read them they contained some of her own ideas, but also mine, and she had a copyright symbol on them, with no mention of my name,
I could have stood up at that meeting and criticised her, but I didn’t want to create a fuss, or embarrass or upset her, so I chose not to.
I wrote an email but decided not to send it, and instead prepare this article on my website.
I have found out that she lives in a suburb near to mine, so she would have had easy access to many state and local newspaper articles and books in local libraries where she could have heard or read about my ideas.
I assume that what she has done, is to try out my ideas, and found that they were successful, and made a few minor adjustments to the methods.
Dr. Bruce Wauchope
I attended another meeting where I purchased a copy of a CD talk by Dr. Bruce Wauchope, and I watched it, to see that some of it was also a description of exercise and lifestyle methods which were an exact copy of mine. I assume that he found the information in modern literature, and thought that it had been put together by a collection of 1000’s of international researchers, and that he wasn’t aware of me, so I phoned him to discuss the matter.
I explained that no-one knew how to treat my ailments in 1975, so I had to study them myself and develop my own methods, and that there were many newspaper articles about it from 1982-3. He then asked me what I did that was different, so I said many things, but one was the concept that patients had a limited capacity for exercise, and that earlier programs which expected patient to keep improving about those limits were failing, and that the methods which I developed would help some patients, which is why all researchers since have had no choice but to copy me, and that the only problem is that they don’t want to tell the public that it was my methods.
He then said ‘so your problem is plagiarism of your ideas” and I said “yes”.
He then said I should get the research paper published, and I explained that I had sent it to two journals including the Australian Medical Journal in 1983-4, but it wasn’t accepted.
He then said that I should contact the journal and get confirmation that they sent the article.
I said that I knew they kept records of published articles, but didn’t know they kept records of all manuscripts that had been sent to them but not published.
He told me to phone them and find out, but I decided to send them an open letter requesting them to publish the article in the next edition of their journal, noting that the original date of the research was 1982-3. See here.
He also told me that a nurse called Kathy was working on the 2nd edition of the guidelines for treating CFS, and I told him that she was probably going to use my methods of treatment because everyone else does, but he then said that he knows the woman, and that she developed the ideas from her own experience.
I said that was highly unlikely, and that she would have read about my ideas, and that I didn’t object to her including my methods as long as she acknowledged me as the developer.
He seemed to be offended by me for saying that, and I got the impression that he had some loyalty or respect for that woman, so I didn’t pursue that aspect, and the conversation ended with me inviting him to keep in touch.
The SA ME/CFS society
I also received the latest edition of the South Australian ME/CFS journal called “Talking Point” (2013 Issue 1). Much of it was discussing my methods of treating the condition, and the problems that international researchers are having, but my name wasn’t mentioned anywhere. Some of the other topics in that journal were also about ideas which I started many years ago. I published my ideas to help other patients, so I don’t mind people discussing them as long as they give me the credit.
Summary
My predicament is this, I developed a method of researching and treating chronic fatigue which everyone else has to use, or they simply won’t succeed, so naturally people have to copy me.
I don’t want to offend anyone who is trying to help other patients, but I know my rights, and it is not practical for me to ignore what has happened.
I don’t know what will happen in the future, but as they say, time will tell.
Adelaide University medical students found cheating in their exams
On channel 9 TV news of 18th November 2013 there was a report about Adelaide Universities 5th year medical students who were using their ipads to cheat in their exams. According to senior lecturer Paul Duggan students cannot be trusted to act in an ethical and responsible manner, but the university takes cheating seriously and will be taking action to stop it.
I would suggest that there are several reasons for the cheating. First of all university students would be more likely to be taught about machiavellian political principles where the objective is to tell lies and cheat to gain positions of power and influence in society, and then write the rules and ignore them, and gain advantage over ordinary people by making them obey them. They then act as if they are respectable, and fake sincerity etc. By contrast ordinary high school student are more likely to be taught about the importance of honesty and rule compliance.
The second reason is that students have seen how Olympic and sporting champions such as Lance Armstrong have been gaining wealth, status, fame and power by being drug cheats, and then, if they don’t get caught they lead lives of luxury, whereas even if they do get caught they can afford to pay lawyers to keep most of their money and get away with the crimes.
Thirdly they would know about my research into chronic fatigue and exercise etc in Adelaide in 1982, and would have seen how Simon Wessely and some of the worlds top researchers have stolen my ideas to gain research funding, promotions, wealth, and fame, and even a knighthood, and how they are protected from criticism, while at the same time they have seen how an honest man like myself has produced those ideas and yet is being treated like scum and ignored.
It therefore doesn’t surprise me that students are following the example of success by cheating.
I would also suggest that if Paul Duggan, and the Channel 9 News team want to discourage cheating they should tell the public about my research, and how it was completed before other researchers began copying it. i.e. they should give credit where credit is due, and not just sit back and watch the liars and copyright thieves successfully cheat their way through life.
An update of The Posture Theory – 2010
The Posture Theory was first published as a three page essay in 1980, and was later expanded to a thousand page book between 1994 and 2000, and continued on this website where I will now give a concise summary in 2010.
Poor posture compresses the chest and abdomen to cause a large range of health problems such as chest pains, breathlessness, and indigestion.
Similar symptoms were seen in nineteenth century women who wore ‘hour glass’ or ‘wasp-waisted’ corsets. It was because the abdomen contains the stomach, colon, liver, kidneys and backbone, and major nerves and blood vessels, and, for example, compressing the blood vessels reduces the flow of blood between the feet and the upper part of the body, Faintness and fatigue occurs because less blood is available to the brain. The women relieved their fainting spells by unlacing their corsets and laying down. However, after many years of wearing corsets some women found that they continued to be fatigued even after they unlaced them or stopped wearing them.
The general range of symptoms is also seen in pregnancy as the womb grows larger and heavier and compresses all of the structures around it, and puts pressure on the veins that come up from each leg and join in the abdomen, and the symptoms are generally, but not always relieved after childbirth as the womb returns to it’s original size and weight.
Therefore any factor which persistently compresses the chest and abdomen is likely to cause chronic symptoms including fatigue.
Nevertheless some patients report that they were fit and athletic up until they contracted a viral infections such as typhoid, malaria, the flu, or glandular fever etc., and that after recovering from the nausea, vomiting and fever, they remained easily exhausted and could not return to their former sporting activities. Their condition has been called a post-viral fatigue syndrome, and various authors have suggested that the virus may have spread to, or affected the brain. The possibilities are that the brain sends less effective autonomic responses to the blood vessels so the flow of blood is weaker, which was previously called neurocirculatory asthenia, or that the virus has infected the nerves, which was previously called neurasthenia, and there is also the possibility that the virus has weakened the muscle fibres, or other structures in the walls of the blood vessels, although there is no firm scientific evidence for any of those conclusions.
Also, another group of patients will report that they were fit and healthy up until a period of anxiety or stress in their life, and that after the stress had finished they continued to be easily exhausted, and were not able to sustain physical effort as before. Some authors have argued that they continue to be anxious but are not aware of it, and refer to their symptoms as an anxiety disorder, and others suggest that the stress damages the brain, or the nerves or the adrenal glands, and refer to the condition as a psychosomatic disorder.
There are many other possibilities, such as changes in the blood chemistry due to an abnormal pattern of breathing, or changes in the autoimmune system etc, but in general the chronic fatigue is due to any factor which affects the quality or flow of blood to the brain, such as poor posture, tight corsets, pregnancy, and viral or stress damage to the nervous system and blood vessels, and of course, those factors would play a part in the other symptoms and the effect would be more likely if multiple factors were involved. The blood carries oxygen and nutrients so the reduced supply of those essentials contributes to fatigue.
There is also evidence that several slightly different syndromes exist with similar or overlapping causes and symptoms..
Ultimately the methods of preventing, relieving, or treating the symptoms involves improvements in posture, wearing loose clothing, immunising against viral infections, and developing a calm and relaxed attitude to all situations.
It is also not practical to consider these ailments as having one cause, or one method of treatment because it isn’t possible to convince a person who has good posture that their symptoms are due to poor posture, or to convince a person who is not anxious that their symptoms are due to anxiety, or that someone who didn’t have a viral infection at the start of their symptoms is suffering from a post-viral condition. M.B
A summary of other factors which cause pressure symptoms
i.e. supporting evidence for The posture Theory
from previous essays
Poor posture, due to spinal deformity or slouching, throws the head and shoulders forwards and puts pressure on all of the structures in the chest and abdomen, and sideways curvature of the spine results in greater pressure on those structures on one side. The amount, type, location, and affect of that pressure is also influenced by the shape of the chest, whether it is shallow or deep, and long or narrow.
Pregnancy and pressure symptoms
The effect can be compared to other factors such as pregnancy where the enlarging womb starts to put pressure on the bladder and bowels and cause such problems as frequency of urination. As the womb continues to enlarge it presses on the abdominal structures and then, in late pregnancy, it pushes against the stomach and heart, causing heartburn, palpitations and faintness, as common symptoms.
|
|
The pregnant womb The enlarging womb of pregnancy causes bladder, kidney, stomach, heart, and lung problems, and fatigue, as it expands during the months of pregnancy. The symptoms are related to the position of the womb and the anatomical structures that it presses upon. Women often notice that their symptoms are caused by, or change to something else depending on whether they stand, sit, or lay on their back or their side. That is because the womb changes position as they move. For example if the woman feels faint in early pregnancy, it is due to pressure on the veins coming up from the legs, so she can relieve it by sitting or laying down. If she feels faint in later pregnancy while laying on her back it is due to pressure on the veins behind the womb, so she can get relief by rolling onto her side. |
|
.
|
The stages of pregnancy In early pregnancy the womb presses on the bladder and makes the woman want to empty her bladder more often. In later pregnancy the womb presses up against the stomach, heart and lungs causing heartburn, palpitaitons, faintness, fatigue, and breathlessness. Toward the end of pregnancy the womb moves down again in preparation for childbirth. The womb can put pressure on the lower veins of the abdomen causing the blood in the vessels of the legs etc to dam up and produce swollen feet, varicose veins, and hemorrhoids. The womb gets larger and heavier in women who bear twins, so the symptoms become more common and more severe, and the problems are more likely to be worse again in women who bear triplets. |
|
|
The shape of the pelvic outlet The normal shape of the pelvic outlet (left) is adapted for childbirth, but is deformed by a stooped posture (centre), or by sideways curvature of the spine (right). |
|
|
The birthing chair Many native women give birth in the squatting position which is a more natural position for pushing and bearing down during labor, and adds the advantage of gravity which made giving birth quicker and more comfortable. Seventeenth century birthing chairs were used to achieve the same advantages but the introduction of forceps delivery in the eighteenth century required women to lay on their back, so birthing chairs went out of fashion. Adjustable birthing chairs were sometimes used in the 20th century to make delivery more comfortable. Reference: The Body Book (1986) page 303 Also reported in my book between 1994 and 2000. |
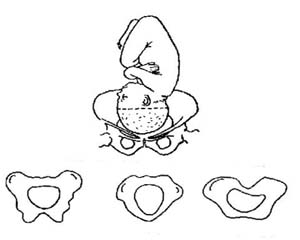
Reference; Cohen ME, White PD (1951). “Life situations, emotions, and neurocirculatory asthenia (anxiety neurosis, neurasthenia, effort syndrome)“. Psychosom Med 13 (6): p.346
Corsets and pressure symptoms
My YouTube video on corsets and related factors can be seen here
Similarly, in previous centuries women wore very tight waisted corsets which caused them a myriad of health problems. Furthermore the low waisted corsets tended to cause ailments related to the bladder, womb, and bowels, such as severe constipation, and some women wore the corsets to induce abortions. The high waisted corsets, by contrast, had a greater effect on the chest, causing chest pains, breathlessness, and faintness. Also the mid waisted corsets pushed the stomach from the horizontal position to the vertical position, and the low waisted corsets pushed the womb from the vertical to horizontal shape, and altered the shape and angle of the pelvic bone and pelvic outlet resulting in such features as shoulder presentation and difficult and painful childbirth
|
Seven different corset styles
|
 |
 |
| In the seventeenth century corsets were made in various styles, and the shape of corsets worn in childhood detemined the permanent shape of her spine and chest in adulthood. | The Countess of Leicester and her children (1596) depicting the late sixteenth century womens fashion which included corsets worn since childhood to permanently alter the shape of their spine and chest by adulthood. See more information about childrens corsets here | Queen Anne of England (1665-1714) wore corsets. She had chronic ill-health, and became pregnant 18 times but only 5 of her children were born alive. |
|
 Most nineteenth century English country farm girls wore comfortable loose clothing and developed broad and deep chests and grew up with the reputation of being, healthy, strong, and robust. By contrast, in places like London and Paris, the women, and some men, wore the corsets which were made in local factories, and sold in the many fashionable city dress shops. Some corsets which had waist circumference of 14 inches were sold off the rack as the minimum standard size, but nowadays the Guiness Book of Records (1962) regards a 13 inch waist as the world’s smallest. They wore the corsets since childhood to deform their chests into a funnel shape in order the give themselves an hour glass figure. They developed a reputation for being weak and sickly, and would faint easily, and suffer from breathlessness, fatigue and indigestion. They relieved their fainting spells by unlacing their corsets and laying in chaise lounges.
Some corsets also compressed the hips and deformed the pelvic bone and altered it’s angle and shape and made childbirth difficult, painful, or impossible.
Poor posture has a similar affect at deforming the pelvic bone. A stooped spine is associated with a longer pelvic outlet, and sideways curvature is associated with various distortions and a flattening of the pelvic outlet, so that it no longer conforms with the shape of the babies head.
Most nineteenth century English country farm girls wore comfortable loose clothing and developed broad and deep chests and grew up with the reputation of being, healthy, strong, and robust. By contrast, in places like London and Paris, the women, and some men, wore the corsets which were made in local factories, and sold in the many fashionable city dress shops. Some corsets which had waist circumference of 14 inches were sold off the rack as the minimum standard size, but nowadays the Guiness Book of Records (1962) regards a 13 inch waist as the world’s smallest. They wore the corsets since childhood to deform their chests into a funnel shape in order the give themselves an hour glass figure. They developed a reputation for being weak and sickly, and would faint easily, and suffer from breathlessness, fatigue and indigestion. They relieved their fainting spells by unlacing their corsets and laying in chaise lounges.
Some corsets also compressed the hips and deformed the pelvic bone and altered it’s angle and shape and made childbirth difficult, painful, or impossible.
Poor posture has a similar affect at deforming the pelvic bone. A stooped spine is associated with a longer pelvic outlet, and sideways curvature is associated with various distortions and a flattening of the pelvic outlet, so that it no longer conforms with the shape of the babies head.
|
Collars, Belts and pressure symptoms
|
Some soldiers were required to wear their belts tight to give a neat appearance. Many such soldiers developed haemorrhoids. The basic cause is pressure on the veins between the rectum and liver. The resistance to the flow of blood damages the veins of the rectum. Another cause is the heavy weight of the pregnant womb, which presses on those veins. Laying on the left or right side etc, can relieve that pressure. A third cause is the lack of fibre in the diet. When wheat stopped being ground by stone, and started being refined in the steel mills, the fibre was removed. The new type of flour was used to make bread which was the staple food, and main source of fibre in the diet. The change to low fibre bread started a world wide epidemic of constipation. Constipation resulted in hard feces which required forced abdominal pressure to empty the rectum, and an epidemic of appendicitis, irritabl bowel syndrome, other bowel diseases, and hemorrhoids. Tight military tunics restrict the expansion and contraction of the chest during exertion. |
see also here Napoleon is depicted in many of his paintings as holding his right hand on his belly, which may have been due to indigestion. When he was young he wore tight waisted trousers which were fashionable at the time. Such garments have the effect of giving a more masculine look by narrowing the waist and making the shoulders look broader by comparison. However, they also tend to push half of the contents of the belly up, and half down, and the head and shoulders incline forward, and the lower abdomen bulges in front like a pot belly. They also increase the pressure on the stomach, which may have caused indigestion. He complained of indigestion later in life, and also suffered from haemorrhoids, and reported that they were aggravated by horse riding. Tight waist belts block blood flow from the rectum to the liver and cause the rectal veins to swell up into a bunch like grapes, similar to the way garters block blood flow in the legs and cause varicose veins below the garter line. (haemorrhoids are varicose veins of the rectum). Bouncing up and down on the back of a horse as it gallops along would put additional and repetitive pressure on the rectal veins, and haemorrhoids were known to be aggravated while riding in a vehicle over bumpy roads. Napoleon reported that his haemorrhoid pain was aggravated while riding his horse to the battle of Waterloo. According to some medical historians he may have won that battle if it was not for the fact that he postponed the attack until the following day to allow his hemorrhoid pain to subside. In the meantime enemy reinforcements arrived and his army was defeated. He eventually died of stomach cancer, and many nineteenth century medical men attributed stomach cancer to compression of the stomach by tight corsets. *** His handwriting has been studied and described with these words . . . “The pressure is firm and dark in appearance”. See here One cause of that would be stooping forward to write, either because of a stooped spine, or poor eyesight where the weight of the head and shoulders is transferred along the arm to the tip of the pen. In some cases the nib actually indents the paper along the line of text. The weight would also need more effort, so the writing would tend to be sprawling scribble. People with straight spines and good eyesight don’t have to lean forward so their handwriting would be effortless, smooth and light, and neat.. See also Napoleon and Napoleon’s influence on French fashion and The Battle of Waterloo Phil Mason was the author of a book called “Napoleon’s Haemorrhoids” . . . According to a review by Medindia.net.news . . .Napoleon was suffering from an acute attack of piles two days before the battle, but his doctors lost the leeches that they used to relieve his agony, and accidentally overdosed him with the painkiller laudanum. He was still suffering from hemorrhoids and the affects of the painkiller when the battle broke out, which stopped him from riding his horse and supervising his troops, and may have been the reason for losing. See here |
Male corsets, including the so-called ‘Military corsets‘ were available for purchace with a variety of other belts and waist constrictors and were used for achieving the v-shaped torso. The cosmetic trick Men with a naturally large chest, have large hearts and lungs, so they look fit, energetic, and healthy, because they are actually healthy. Men with smaller and narrower chests wanted to look athletic and healthy, so they constricted their waists to make the chest look large by comparison. Unfortunately they still had small chests, and by making their waists smaller, they were crushing their already small hearts, lungs and stomachs, and although they looked healthy, they were actually making themselves less fit, less energetic, and more prone to illness.
|



Some other forms of clothing produce pressure symptoms, such as high heel shoes, which lift and tilt the pelvic bone, increase the arch in the lower back and neck to cause back and neck aches, and where military uniforms included tight collars, such as “the Choker“, the pressure obstructed blood flow to the brain and soldiers were more prone to faintness in battle, and where tight belts were part of the uniform, large numbers of soldiers developed hemorrhoids.
In general terms any factor which puts pressure on the body causes strain, and impairs blood flow, resulting in local or widespread symptoms and ailments. e.g. when a person crosses their legs the pressure on the blood vessels of the thighs impairs blood flow to and from the feet, and when a tornique or blood pressure cuff is placed on the arm, the increasing air pressure in the cuff puts pressure on the blood vessels, initially restricting blood flow, and if continued, blocks the blood flow completely.
THE POSTURE THEORY AND DA COSTA’S SYNDROMEThe Posture Theory explains the cause of many health problems, but more specifically, it is a way of explaining the cause of chest pains, palpitations, breathlessness, faintness, and fatigue which occur in the absence of any evidence of heart disease. Those symptoms are characteristic of a common medical condition known as Da Costa’s Syndrome which was named after Jacob Mendez Da Costa who, in 1871, was the first medical researcher to note that they seemed to occur as a set in many individuals. Those symptoms can occur at any time, but particularly during exertion. Therefore The Posture Theory is essentially a way of explaining the symptoms of Da Costa’s Syndrome which could perhaps, in relevant cases, now be referred to as The Posture Syndrome. Da Costa’s original 1871 research article Da Costa’s reported his observations of almost 300 patients, and provided the basis for the diagnostic criteria which included the typical features of chest pain, dizziness, breathlessness, palpitations, and fatigue that were associated with a poor physique, a thin chest, marching at double quick pace, hard field service, and viral infections, and he noted that the waist belt of the knapsack seemed to be aggravating the symptoms. The pulse was influenced by position, such as stooping, laying on the left and right side in some cases, and the back in others, and the condition was relieved by improved physique. Recommended treatment included not wearing clothing which constricts. Reference: Da Costa, J.M. (January 1871) “On Irritable Heart,” The American Journal of the Medical Sciences |
||||||
The Cause and Nature of the Symptoms of Da Costa’s Syndrome |
||||||
Neck ache, and lower back pain These symptoms involve a dull ache in the neck, or sharp pain in the mid neck, or sharp pain between the shoulder blade and the neck, or cricks in the neck, and dull aching in the lower back. They occur because a stooped spine (kyphosis) throws the weight of the head, shoulders, and chest forward to put a mechanical strain on all of the bones, muscles and ligaments of the spine. Furthermore, when the upper spine is stooped the neck is more arched than usual, disposing to neck ache, and any scoliosis, or sideways curvature of the spine will put more strain on one side disposing to aching at the spinal joint central to the curve. That can in turn dispose to aches, numbness, pins and needles, or other sensations in the shoulder, arm, and muscle relating to the nerve coming from that side of the neck joint. There may also be a compensatory increase in the forward and sideways curve of the lower spine which can increase the mechanical strain and incidence of low back pain.
|
||||||
|
Lower left-sided chest pain – The most typical pain is a sharp stabbing sensation occurring perhaps 2 or 3 times in a year (or more rarely) in the lower left side of the chest, and is probably due to postural strain on the structures between the ribs which produces a tendency to the pain. It may occur at any time when sitting relaxed or standing, and it feels as if a 3 inch sewing needle is suddenly stabbed in and out of the ribs and is over within a fraction of a second, as if a nerve has been pinched. It’s occurrence on one side of the chest is probably related to sideways curvature on the spine (scoliosis) placing more pressure on one side, and stretching the ribs apart on the other, and it occurs on the opposite side of the curve. It occasionally occurs on the right side as well. There is also a dull ache occurring in the same location, and is probably due to strain from the pressures of constant posture, but the pain does not actually occur except when running, and then only rarely. When it does occur, it happens every time the persons foot touches the ground, so that the ache may be felt 100 times in a one hundred yard jog along beach sand. The third type of chest pain occurs in the extreme left side of the chest, and is due to severe cramp in the muscles of the chest under the arm. It is equivalent to severe cramp in the calf muscle of the leg. It has been described as being brought on by muscular effort, such as cranking a car engine, in which case it is on one side of the chest related to which arm was used to crank the engine. Exactly the same pain can be felt on both sides of the chest where it is brought on by prolonged laughing, and it may be accompanied by difficulty breathing, because inhaling expands the chest and stretches the muscles and aggravates the severity of the cramp. The cramp will also be made worse by trying to lift or move an arm because such movements also stretch the muscles of the chest, so that the person has to stay in a semi crouched position, and the pain will cease only when laughing stop. According to a website called About.com Orthopedics, inflammation of the rib cartilages can be caused by repetitive pressure on that area of the chest, which is seen in some athletes, such as competitive rowers. The inflammation of the ribs is also called ‘costrochondritis, and Tieze’s syndrome. See here – such athletes lean forward repetitively, in a similar way that clerical workers lean forward to read and write at a desk. See my diagram here. Breeches of my copyright See also costrochondritis here, and my report on the copyright theft of my observations and ideas about cause here. |
||||||
|
Palpitations of the heart – This symptom involves the perception of the heart beating in combination with it tending to accelerate and pound faster and faster in an alarming way which does not seem to slow very easily. It can occur at any time of the day or night but often just after laying down to go to sleep. The problem seems to relate to laying down in the normal way, but can be prevented by laying down on the back slowly and resting with the head slightly raised on three pillows for a few moments, and then removing a pillow, and resting on two, and then one. The gradual movement backwards seems to offset the symptom. The problem also seems to be worse in any situation where the pulse rate is likely to increase such as when a person is anxious just before standing in front of an audience to give a speech. There are probably three factors contributing to the symptom. The first is the curved shape of the upper spine, the second is the shape of the chest, and the third is the shape of the heart. The heart and ribcage can be compared to a bird in a bird cage. If the birdcage is large then the bird can flap its wings comfortably, but if the bird cage is small then its wings will bang against the wire frame of the cage, and if a person has a small ribcage, then the beating heart will pound against the chest wall and be more easily noticed. If the person becomes worried that there is some indication of heart disease then the worry will accelerate the rate and make the problem worse. The perception of heartbeat can also be compared to the pulse rate which no-one is aware of until they place their fingers over the artery in their arm. With slight pressure on the fingers nothing can be noticed, but by pressing the fingers against the artery its wall can be felt each second as a pulse of blood passes through it. Similarly if the heart is squeezed into a small chest, then its beating may be more readily noticed each time it pounds against the chest wall. Similarly people with broad and deep chests and rib cages have hearts which are pyramid in shape and they would sit stable in the chest, but people with long narrow or flat chests tend to have bowling pin shaped hearts which would tend to wobble about when beating fast, and that would produce a different and perhaps more alarming sensation. Consequently the palpitation may be felt when a person lays down at night because, as they lay back the curve of the upper spine straightens out and drags the front of the chest backwards and compresses it against the heart, so that its beating can be felt. That may explain why the symptom can sometimes be prevented by laying back slowly. or by sleeping in a semi-sitting position with the head raised and the spine remaining curved in a C-shape to maximize the size of the chest space. The palpitations may also perhaps relate to excess amounts of blood pooling in the veins of the legs, so that when the person lays on their back, the sudden removal of the gravitational load on the blood causes and excess volume to flow toward the heart chambers with temporary greater force. In other respects such patients, and anyone else who has problems with a pounding heart when giving speeches, the symptom can be prevented or relieved by having a small glass of wine a few minutes earlier to relax the heart muscle (alcohol is a muscle relaxant which passes immediately through the stomach wall to the heart muscle nearby). It may also be useful to take a few slow, regular, and deep breaths to stabilise the position of the diaphragm which the heart sits on, and to use a prepared speech, so that the element of doubt is removed from the talk. NASA I developed these ideas more than 30 years ago and have been improving them ever since, because they are effective. Recently, on a Channel 9 TV morning news programme it was reported that astronauts returning from space flights had a problem with faintness. A spokesman from NASA attributed to the lack of gravity in space. They had developed a new method of treating the problem which involved exercising on a stationary bike with their head and spine tilted back, and said it was effective because it reduced the effect of gravity on the blood in the body. Their ideas are essentially the same as some of the ideas that I developed. See more in the faintness section here This is a quote from the Medical Unit, or the abc NEWS website “The exercise program is intended to help the heart grow in some patients and in others to condition the heart muscle and prevent fainting. “It involves exercises that avoid gravity,” Jaeger said. “And for the first time ever we actually have a way to turn around the person’s symptoms and actually cure them.” For Chandler, the prescription is simple. She eats salty food to keep her blood pressure up, tilts her bed when she sleeps to keep her blood flowing, and she exercises on a recumbent bike. “I actually bought a recumbent bike,” she said. “I will be using that more often now to build up my heart muscle. I want to be at my best.” Chandler and some others are now free from fainting spells, thanks to a little help from “The Right Stuff.” See here (Note that in some people where the cause has been short term, such as astronauts, the condtion probably is curable, but for many people the ailment is not due to a temporary or long term lack of exercise, and is manageable, but not curable). Leaing forward is the cause, leaning back is the cure According to my theory it is repeatedly leaning forward which compresses the air in the chest and strains and damages the blood vessels below the chest that eventually causes faintness. According to NASA the cure involves exercising while laying back on a recliner bike, which takes the load of gravity of the blood.
|
||||||
|
Breathlessness – This symptom takes the form of an air hunger where the person takes a full and deep breath until inhaling reaches its limit and can’t go any further. However they still feel as if they have not got enough oxygen so they forcibly attempt to breath even more deeply, like a forced yawn, and then they have to take another two or three full breaths in quick succession. The person then breaths at a normal rate for a few minutes and may then have to reach for breath and forcibly inhale again. Occasionally the person may bend at the hips, place their hands on their thighs, and arch their back and expand their chest to inhale with greater force and effectiveness.The symptom may occur every few minutes or every few hours or only once or twice a month, and may occur at any time of the day or night, regardless of whether the person is sitting, standing, or resting, or laying, and it occurs more frequently in cold weather, and more often when walking, especially up a hill, and much more often when slowly jogging, in which case the quick successon of forced breaths may be required as often as every 10-50 yards. see also here, and : ref 22 Wolf S. 1947 There is sometimes a slightly different but similar symptom which involves the need to take deep yawns. The symptom is also aggravated by wearing any tight clothing which restricts the expansion of the chest during the inhalation phase of the breathing cycle. For example having a snugly fitting and inflexible belt strapped around the chest can cause extreme respiratory distress during the inhalation attempt. The breathlessness can also sometimes be caused by leaning toward a desk or bench which involves bending at the waist or rib line. That type of bending pushes the breastbone backwards and compresses the chest and abdomen, and restricts the upward and downward movements of the diaphragm, thereby restricting both the chest and abdominal phases of breathing, so the symptom probably results from an anatomical strain or damage brought on by many years of constant or repeated compression of the lungs or diaphragm. The postural pressure may have damaged the lungs so that the amount of oxygen passing from the lungs to the blood stream is impaired, or it may have damaged the diaphragm (the main breathing muscle) and altered its natural and normal function. The exact anatomical basis for the symptom is not clear. A related feature of Da Costa’s syndrome is CO2 intolerance, and also, distressing symptoms are brought on by wearing a gas mask, and it probably relates to the confined space of the mask, and the build up of excess vie CO2 in that small space. With normal breathing in fresh air, the CO2 dissipates immediately. This is a quote from J.M.Da Costa’s original research paper of 1871 page 25 . . . “it was astonishing that the respiration was so little hurried. And, as a general rule, it may be stated that this curious disorder presents the anomalous condition that increased action of the heart does not give rise to increased frequency of breathing; we find in it a peculiar pulse respiration ratio.” (end of quote) He then cites some examples of me with pulse rates of 124 and respiration of 25, and pulse of 146 and respiration of 26, and pulse of 192 and respiration of 26, and he gives one exception to the rule.”(end of quote) (Some authors make the mistake of thinking that this symptoms is panic induced hyperventilation)
“All crooked or constrained bodily positions affect respiration injuriously. Reading, writing, sitting, standing, speaking, and working with the trunk of the body bent forward are extremely hurtful by overstretching the muscles of the back, compressing the lungs, and pushing downwards and backwards the stomach, bowels, and abdominal muscles.” Reference: George Black, M.B., Edinburgh, (1910), The Doctor at Home and Nurse’s Guide-Book, revised edition, Ward, Lock & Co., Limited, London, Melbourne and Toronto. pages 77-78. |
||||||
|
Faintness and dizziness – The type of faintness is a sense of light headedness, and a feeling as if about to lose consciousness and fall to the ground, and it can be associated with unstable or low blood pressure. Some patients do actually faint from time to time, but others often feel a sense of faintness but never actually lose consciousness, and the symptom may be slightly or much more distressing than any normal sense of faintness, and occurs in response to minor, or sometimes very slight movements of the body. Sometimes there is another sensation, especially with rotation of the body, of an odd and distressing sensation in the chest, as if the heart is about to stop beating. The faintness most commonly occurs when getting out of bed and standing up suddenly in the morning, (orthostatic intolerance) and can be prevented by getting up slowly, and first sitting on the side of the bed, and then standing slowly and walking off at a casual pace. The symptom may occur throughout the day at any time especially if the person gets out of a seat and stands up suddenly, rather than slowly, and it may be a more or less constant feeling, or occur several times a day or a week, or several times a month. It may also occur when the person leans forwards at a desk and in very extreme cases if they lean forward to write 10 times, they will feel faint each time, and sitting up and leaning back slightly each time will relieve the faintness, so the sense of faintness comes and goes 10 times, and continues in that manner until the person stops repeatedly leaning forward. (note: scroll down to fig.15 for a leans forwards at a desk link which reports on corsets, leaning forward to write, and scientific pressure measurements in 1887). The problem is greater if the person is squatting as they lean forward. The faintness also occurs whenever the person is subjected to centrifugal forces such as when they are a passenger in a car which speeds around a curve in a country road, or if they are a passenger in a swirling amusement park ride, or on an up and down or winding roller coaster, and in fact, many patients avoid such entertainment activities altogether. It also occurs when a lift in a tall building accelerates to start its upward journey, and decelerates to stop, and in a plane which accelerates at the start of its flight , or suddenly drops in a down draught, or decelerates to land. The symptom also occurs sometimes to an extremely alarming degree when a patient is placed on a tilt table, and it is moved up and down and rotated sideways at various angles to get different X-ray images of the patient. The symptom is due to a weakness in the circulation of blood in the body (hence the term neurocirculatory asthenia) and is often seen to a minor degree in many fast growing teenagers who have a condition called sway back, probably because that posture puts pressure on the chest or kidneys. However many teenagers grow out of their sway back and the symptom becomes a thing of the past, but in other people it starts in adulthood and takes a more persistent course. It is also more common with people who have a stooped upper spine and a flat chest, probably because the downward postural pressure on the chest impedes the blood flow from the legs to the heart and brain. That constant pressure may actually stretch all of the blood vessels below the waist so that they become more elastic, or so that there is an abnormally disproportionate amount of the bodies blood below the waist which is more subject to being displaced by any type of gravitational or centrifugal force. To a lesser extent this is evident as orthostatic hypotension related to varicose veins below the garter line of the leg, where pressure impedes the upward flow of blood and damages the tone of the leg veins so that blood tends to pool in them and be delayed in it’s return to the heart when the person stands up suddenly. The faintness is also likely to be a problem if the person wears a tight collar which reduces blood flow to the brain, and can be relieved by loosening the collar, and was very common amongst nineteenth century women who wore tight waisted whalebone corsets. Those women routinely relieved their fainting spells by unlacing their corsets and laying on their backs with their head and shoulders slightly elevated on the arm of a chaise lounge, in the then common fainting rooms, A similar beneficial effect on spinal posture and the symptom can be achieved by laying in a modern recliner chair tilted slightly back. A milder from of this could be the orthostatic hypotension caused by wearing leg garters which results in varicose veins below the garter line, where excess blood pools, and is delayed in it’s upward flow when the person stands up suddenly, and which occurs because those veins have lost the strength to respond appropriately. The symptom of faintness or dizziness in Da Costa’s syndrome would also occur in response to any gravitational or centrifugal force acting on the body, except much more readily and severely, which is why such patients avoid entertainment activities like roller coaster rides, whereas healthy people find the experience exciting and enjoyable.. The dizziness is a slightly different sensation which sometimes involves a sense of obscure fuzzines at the back of the head in an area just above the top vertebrae of the spinal colum, and or, a sensation of the inside of the head, or the outer walls and ceiling of a room swirling, but not always, and it seems to occur as a mixture of dizziness and faintness, with a sense of being about to lose consciousness. It is most commonly brought on by bending the neck back to look up at items on tall cupboards. It is probably the result of that neck position putting pressure on the blood vessels in the neck and interfering with the efficiency of blood flow to the brain. Dizziiness also occurs to a more significant degree than normal with rotational movements of the body. This is probably because, with normal posture, the head is balanced directly above the spine, but when a person has a stooped spine the head is thrown forward by at least six inches forming a radius about the spine, and therefore the outer extreme of the head turns in a large circle with a diameter of at least twelve inches, thereby throwing blood outwards from the neck with greater centrifugal force. Therefore, in persons with an abnormal stooped curvature in the upper spine, the dizziness can be relieved or minimized by deliberately forcing the spine to be straight and thereby positioning the head directly about the spinal colum with the head more slowly rotating about the spin of the feet. The dizziness may also be partly due to a weakness in the blood vessels below the chest where some of the blood in the lower body is thrown excessively outwards with the spin and reducing blood flow to the brain.
|
||||||
|
Fatigue related to sleep problems and exercise limitations – Some patients report that they have suffered from fatigue for as long as they can remember so they were probably born with the problem, and some report that they know that they are now troubled by fatigue, but they cannot recall any particular time or incident when it started, and others report that it started over a period of time (months or years) when it seemed to gradually get worse without being particularly troublesome until it became so severe that they had to rest, and that they had to rest for months or years to recover, and that they never fully recovered . They may in fact report that the fatigue accrues in an obscure way until they reach a state of extreme exhaustion again, and the process of recurring severe exhaustion may happen three or four times over a period of a decade before they decide to restrict their lifestyle as a means of preventing the relapses. The fact that the fatigue does not respond in the expected manner of being relieved by rest or sleep and the fact that it tends to accrue over a period of weeks or months is one of its significant differences from normal fatigue, which a person can easily recover from by getting a good nights sleep etc. During the development of the ailment the instability of blood pressure, breathlessness, faintness, and dizziness, and fatigue seem to occur as a linked sub-set of Da Costa’s syndrome. In the extreme case the fatigue involves restlessness, wakefulness, the inability to sleep for days or weeks at a time, but later waking up several times at night and not being able to get back to sleep again, and waking up tired, and tiredness occurring several times throughout the day are features. The tiredness sometimes but not always responds properly to rest, and has the characteristics of a sleep disorder. The symptom has sometimes been derogatorily referred to as TATTS (tired all the time syndrome), which reflects ignorance about the different qualities in the nature of the symptom, and the sometimes profound severities of the condition which bare no resemblance to normal tiredness, and continues to produce confusion in diagnosis. The bouts of fatigue may occur for weeks or months undiminished, because there is no effective treatment or medication for the problem, other than long term rest, mild exercise, and the passage of time, which is why many patients avoid the factors which induce them, and lead generally quiet and moderate lifestyles. There is also an exercise disorder where the person is so weak that their heart may pound each time they lift their foot of the ground as they walk slowly along the street. They may be walking or jogging last in exercise training programmes and have to reach for breath several times each 20 yards or so, and if they exert themselves suddenly or sprint fast their heart will pound violently and they will feel faint and dizzy and fall to the ground and crawl about restlessly because restricting their movements causes extreme physical distress inside the chest. Consequently they have to give up the sporting activities that they have participated in regularly in the past, and, because of the distressing nature of the symptoms, most of them refuse to participate in remedial exercise programmes, or drop out of the course soon after starting. The fatigue seems particularly linked to the faintness which occurs when leaning forward, either toward a desk, a bench, a washing machine, or the kitchen sink etc. As another example, in order to clean low windows on a house it is necessary to squat down and lean forward. Each time the person leans forward they feel faint, and if they choose to ignore the problem and keep repeatedly leaning forward until all of the windows are finished, and then stand up, they may feel faint and weak and exhausted. After only that half an hour of minor effort in the morning they will have to spend the entire afternoon resting in bed, and may still be exhausted when they wake up the following day. The link between faintness and fatigue probably occurs because leaning forward compresses the chest, heart, and lungs, and then the increased air pressure in the lungs impedes blood flow from the feet to the brain. In that regard there is an experimental procedure called the Valsalva’s Manouver which is used in scientific laboratories to artificially produce the symptoms of stress in the absence of any psyhological factors. When this manouvre is being used the patient is asked to pinch their nose shut, and keep their mouth closed and exhale with force. As the air cannot escape from the lungs the pressure builds up and impedes the flow of blood from the feet to the brain. The brain and nervous system then react with a reflex that stimulates and contracts the blood vessels of the legs, which increases the blood pressure to force the blood to go upwards through the compressed vessels in the chest. Hence there is a relationship between air pressure in the lungs, the nervous system, and blood pressure. >Consequently if a person was constantly or repeatedly leaning toward a desk or bench for many years they would also be blocking blood flow from the feet to the brain and putting a lot of pressure on the blood in the veins below the chest. Such long term pressure might affect the tone of the walls of those vessels, or gradually damage them, and weaken the upward flow of blood, and become a disorder of circulation (i.e. vascular dystonic circulatory asthenia). In fact this form of fatigue has been called neurocirculatory asthenia – a weakness of circulation, and neurocirulatory dystonia – a disorder of circulation due to abnormal tone in blood vessels). The weakness of blood flow to the brain would account for poor concentration, poor memory, and problems with wakefulness and sleep which are all common in DaCosta’s syndrome. Furthermore the weakness of blood flow from the feet to the heart would account for the faintness which occurs when standing up suddenly, or when standing up from a squatting position, and it would also explain the weakness in the bodies response to sudden, vigorous, or rapid exertion. Hence there is a link beween posture, sedentary work, constantly or repeatedly leaning forward, Valsalva’s maneuver, and transient, recurring, prolonged, or chronic symptoms of tiredness, faintness, and physical exhaustion. The condition is common in sedentary town workers, and rare in country farm laborers.
|
||||||
The Abnormal Response to Exertion, and it’s possible relation to Abnormal Sighing Respiration ©In Da Costa’s syndrome there is an excessive tendency to sigh which occurs at variable intervals, but it sometimes takes the form which can be explained as if there is a standard depth and rate of breathing and oxygen absorption into the lungs which is not being achieved, for one reason or another, so the person tends to take an extra deep breath every few minutes to make up for the lack of oxygen consumed during that time. Sometimes the inhalation needs to be forced to achieve the depth of breathing required to make up for the deficiency, and sometimes two or three forced deep breaths may need to be taken in quick succession. The need to take the extra sighs may occur every few minutes, or several times an hour or day, or month, and is more frequent during cold weather. This becomes more noticeable with exertion such as slow jogging where a normal healthy persons breathing rate, volume and absorption increases according to the extra amount of oxygen required for the exertion. However with the type of breathing pattern seen in Da Costa’s syndrome it sometimes seems as if the breathing process does not properly increase to meet the extra requirements for the effort of jogging, so that they may accumulate a greater oxygen debt and need to take two or three extra forced deep breaths every twenty yards or so. The same problem seems to occur with sudden rapid sprinting but to a much greater extent. The healthy persons breathing pattern adjusts to the oxygen requirements, but with Da Costa’s syndrome it seems as if the respiratory mechanism is slow to adjust, so that after only twenty yards the person may fall to their knees repeatedly gasping for breath, with their heart pounding in their chest, and feeling faint, dizzy, and excessively restless, and crawling about with extreme exhaustion for 15 minutes or more, and be fatigued to a lesser extent for a week or more, before resuming milder forms of exercise. It may be a matter of the respiratory reflex not working properly so that as the level of exertion increases the breathing becomes shallower or the oxygen absorption less, so that an oxygen debt builds up until the person feels an obvous need for more air, and then forceably inhales to get the extra oxygen required. The explanation may not be entirely correct in every detail, but it is close enough to portray the difference between the healthy response ot exertion, and the Da Costa syndrome response, and it may or may not be due to a fault with the thoracic diaphram, or the autonomic nervous systems regulation of breathing, and it may due to an abnormality of breathing pattern rather than too much or too little, or to inefficient respiratory efficiency which is worse as the level of exertion increases, and many people with this problem were former athletes who use exercise as a possible means of improving their fitness to recover from the fatigue, so it is not due to a fear of exercise, and it can occur when the person is otherwise relaxed, so it is not due to an anxiety state, and it is probably not due to any disease of the heart. The purpose of this explanation is to provide a conceptual way of understanding the differences between the normal response to exertion, and the DaCosta’s syndrome response, where the difference is otherwise not recognised, or is trivialised, or misinterpreted etc. It is subject to being tested or disputed or to someone else coming up with a better way of explaining the difference. This explanation was posted on this website on 4-2-08. When referring to this explanation please cite this website as the source, See also: Low oxygen consumption and low ventilatory efficiency during exhausting work in patients with neurocirculatory asthenia, effort syndrome, anxiety neurosis, . . . See also (re: the respiratory disorder is different to hyperventilation) – Hyperventilation and chronic fatigue syndrome . . . and . . . The chronic fatigue syndrome and hyperventilation |
||||||
|
Upper abdominal pain – also called epigastric pain. The primary symptom is a dull ache of varying intensity occurring periodically and occupying an area the size of a 20 cent piece in the mid upper abdomen just below the tip of the dagger shaped breastbone, or sternum. The pain is probably related to slouched posture, sideways curvature of the spine, and chest shape, Poor posture pushes the breast bone downwards, sideways curvature alters the angle of the breastbone, and a flat or funnel shaped chest involves a breastbone which is vertical or receding. Hence when a person with such features leans forward the pointed tip of the dagger shaped breastbone is pushed downwards, backwards, and sideways with a twisting motion into the area where the food pipe joins the stomach, Such repeated action would make the valve like junction sensitive to irritation, and be likely to allow small amounts of stomach acid into the lower end of the food pipe, and possibly also weaken the ligaments and muscles in the area permitting occasional sliding hernia. It might also compress the outlet of the stomach where it joins the duodenum, or partially rotate the stomach and twist it’s outlet and block the flow of gastric acid, which would therefore build up to an excess degree in the stomach and cause tenderness and pain by irritating the stomach wall, and in prolonged cases result in the formation of lesions and peptic ulcers. See also ulcers. Regardless of the cause, the pain is induced by repeatedly leaning forward for an hour or more, and when induced it is aggravated by very minor postural movements. For example it may then be aggravated by leaning forward to tie up shoe laces, in which case the person should buy moccasin style, or slide on shoes which can be put on without bending. The abdominal pain is also aggravated by wearing tight belts about the waist, or tight elastic bands on underwear, so loose clothing should always be worn, and loose waisted trousers can be held up by shoulder braces or suspenders, rather than belts. Sometimes the pain is simply caused by the belt pressure, and sometimes because, when the person slouches the pressure from the belt resists the downward movement of abdominal contents, so they are squeezed from above and below when the person leans forward. On some occasions the relation to pain is obvious but it is usually obscure, subtle, and delayed. The more the pain is aggravated the worse it gets and the longer the abdomen remains tender to the slightest touch. By aggravating the problem for an hour the pain may persist for several days, and by aggravating it for two or more hours the pain may persist for weeks, and any strong strain on the abdomen, as from digging forcefully into the garden and jolting the abdominal muscles can make the pain persist for months. The pain is also aggravated by stretching the arms upwards or sideways, because the arm muscles are connected to the chest and abdominal muscles and drag on the diaphragm and the junction of the stomach and food pipe. The pain can be influenced by some foods. Acid foods such as lemons and oranges, and also spicy foods should be avoided. Also the problem disposes to constipation, so high fibre foods should be included in the diet to keep constipation to a minimum, but even some hight fibre foods, particularly cabbage, and legumes (peas, beans and peanuts), should be avoided because they can also aggravate the pain. If the pain is aggravated in the morning, it may subside in the afternoon, but commonly it may recur and awaken the person at 2.a.m. in the morning perhaps because the periodic peristaltic flow of food residue at night may pass the area of pain and the bulging bowel may nudge the tender area and produce the pain. (Similar to the way in which an egg produces a bulge in the outer surface of a snake as it passes through the inside). The irritation of that area of the abdomen is near the solar plexus and some aspects of the ailment suggest esophageal achalasia (faulty function of the valve like structure joining the food pipe to the stomach). The fact that the severe pain can sometimes be accompanied by difficulty swallowing and can be relieved by a drug called Somac indicates the probable involvement of heartburn due to more significant leakage of acid, and the fact that it is often accompanied by severe constipation and multiple pains and cramps in the bowel, indicates irritable colon may be an additional or secondary problem. It is therefore best to prevent the problem by developing good posture during childhood. The pain can be relieved by laying in a recliner chair, especially a dentists chair which is shaped to push the lower abdomen forward and allow the upper abdomen to arch up and take the tip of the breastbone outwards away from the stomach. If the pain is only mild it can often be completely relieved by laying in such a chair for only half an hour, but if the pain is severe then such rest will only produce slight relief. Laying in bed on the back also relieves the problem but in severe cases it may be necessary to raise the head and lift the knees as well to take all pressure of the abdomen. As previously mentioned, it is also useful to always wear loose clothing, avoid acid foods, include fibre in the diet, and sometimes, if difficulty and pain swallowing food or water is present, the drug Somac can be beneficial. (Gastric reflux is another name for heartburn and is the most common symtom of pregnancy and it is caused by the enlarging womb pressing up against the stomach, and women report that laying down, stooping, or bending brings on attacks. It is relieved by laying on the back with the head and chest slightly elevated).
Other types of abdominal pain occurs because the lower ribs and the lower rib (or costal) cartilage of the rib cage press and dig back into the liver and colon and that process then pushes the structures behind them against the back ribs. Consequently there may be tenderness or soreness in the muscles and anatomy on the left and right side of the front of the chest at, or just above or just below the lower rib line, and a variety of pains along the track of the transverse colon, especially on the extreme left or righ sides, and tenderness or soreness in the left and right kidney area and the back muscles at the same level of the torso. Pain occurs whenever an anatomical tubular structure is blocked because a biological reflex makes the preceding section of the tube go into spasm in an attempt to squeeze the contents forward with greater pressure in order to force it past the blockage. Hence a lot of pain will be experienced if a kidney stone blocks the ureter tube which drains it, and similarly sustained postural pressure on the bends of the colon may start a sequel of blockage, spasm, and pain. Severe abdominal pains: After being aggravated by such minor problems as leaning forward repeatedly , or jarring the stomach while digging in the garden, there may follow a period of several months of severe pain. During those periods the pain remains unabated from day to day for weeks or months until it eventually subsides with time, and may be accompanied by severe constipation, severe bowel cramps, multiple sites of diverticula pin head sized pains along the entire track of the colon, sore or frank protruding hemorrhoids, constipative evacuations which on some occasions tear and put split lesions in the ring of the anus to produce bright red streaks of blood in the excreta, and muco-membranous colitis with the passage of opaque slithers of the gut lining. Those pains do not respond effectively to any form of treatment or medication, which is why many patients avoid the minor aggravating factors as a means of prevention. However, in most cases, even when the symptoms are severe, there is still no x-ray evidence of disease, so many doctors trivialise it and treat it as if it is mere indigestion because they either don’t believe, or can’t understand or comprehend what the patient is complaining about. The condition is not, or rarely associated with, or aggravated by anxiety, and can occur, and persist when a person is perfectly calm. The abdominal symptoms are associated with and, or involve varying degrees of colon spasm which is referred to as Irritable Bowel Syndrome, and were previously regarded as psychosomatic disorders involving “learned Illness Behavior” until the discovery of bacterial and other abnormalities in the colon in the 1990’s. Since then that diagnostic criteria has not been applied to this category of illnesses, and by association are not applicable to the other symptoms of DaCosta’s syndrome. See:(IBS 4.1, 27-12-07). |
||||||
|
Kidney ache – This is a dull ache in the area behind the kidneys, either in the back muscles or the kidneys themselves. It can occur after sitting at a desk and leaning forward for several hours and starts on one side, but if the activity continues the ache will start on the other side as well. It sometimes seems to be followed by alterations in urinary function and the development of kidney stones. The ache is also brought on by exposure to cold breezes which is why it occurs more often in winter. As a general rule winter produces cold breezes and summer produces warm air, but sometimes when walking in summer with a cold sea breeze blowing on the back the chill in the breeze will make one kidney ache, and soon after the next, and once induced the aches will persist for days or weeks after. This problem can be prevented by wearing a padded vest over the kidneys. The effects of pressure on the kidneys is evident by the fact that people who are having kidney x-rays are required to have a dye injected in their blood so that the trace of the dye passing through the kidneys to the bladder will show up on the image. Patients are asked to lay flat during the x-ray procedure, because, if they slouch, the postural pressure will compress the kidney sand their tubing and interfere with the flow of the dye. When Benjamin Franklin was 80 years old he had problems with kidney or bladder stones where he wrote “my sitting at the desk had already almost killed me” and “the stone gave me much pain, wounded my bladder and occasioned me to make bloody urine” and said “when I attempted to write the pain would interrupt my train of thinking” and that he had good health except “being only troubled with the stone which sometimes gave me more than a little pain and prevented my going in a carriage where there are pavements” and sometime later he even had trouble with the pain when standing or walking. (when a kidney stone blocks a hollow tubular structure the walls of the tube go into powerful and painful spasm in an attempt to force the fluid within it past the blockage. Pain occurs if the stone doesn’t move and the pressure increases. Postural pressure which occurs when leaning toward a desk would increase the pressure in the fluid, as would the bouncing up and down action of a carriage going over potholes etc, or in severe cases the simple act of lifting the feet up and down as the person walks could have a similar effect. |
||||||
A summary of The Posture Theory and Da Costa’s SyndromeThe symptoms described above are more consistent to those of Da Costa’s Syndrome than any other ailment. When studying the symptoms individually there were a lot of apparent differences which sometimes seemed contradictory. For example, the faintness could be caused by standing up suddenly, the dizziness by bending the neck to look upwards, and one of the chest pains could be caused by cranking a car engine, and another type by jogging up and down along beach sand. The stomach pain could be caused by wearing a tight belt all day, or by tieing up shoe laces, and was more likely to occur in relation to various foods in the diet, and the kidney ache could be brought on by exposure of the back to cold breezes. The breathlessness is more likely to occur when jogging, the palpitations can be relieved by a glass of alcohol, and the fatigue involves problems with sleep and exertion. However, there is one factor which is common to all of those symptoms, and that is that at some time or other, in some way or other, they could all be caused by leaning forward, particularly in activities which require repeatedly leaning forward. Most people are involved in activities which require them to lean forward but they don’t get such symptoms and that is because, most people have reasonably straight spines and reasonably deep chests. By contrast patients with DaCosta’s syndrome are typically thin and stooped and they have flat chests. It is their physique which causes the problem because when they lean forward their torso bends at the lower rib line and the breastbone is pushed backwards. Consequently when they lean forward they strain their spine and compress their chest and abdomen and everything within to cause the main symptoms of chest pains, palpitations, breathlessness, faintness, and fatigue, and many others not so typical or so commonly seen. Essentially the symptoms are disposed to – and, or- caused by any combination of factors which compress the chest, and restrict it’s size, and thereby compound the mechanical pressure on the rib cage and chest cavity, such as a stooped spine, and small and thin chest, and in some cases, the enlarging womb of pregnancy, and tight waist bands, belts, or corsets, and are more likely to occur in any long term activity which involves repeatedly leaning forward. Hence the study of those symptoms became a study of DaCosta’s Syndrome, and then The Posture Theory, and then the theory became a study of Posture and Health. |




The typical face, build, and posture of Da Costa’s Syndrome
Also called the Effort Syndrome, and nowadays a main type of Chronic fatigue syndrome
|
Typical The typical characteristics of something usually refers to those which distinguish it from others, or those which are most commonly encountered. It therefore didn’t surprise me when I read that the typical Da Costa’s syndrome patient had been described as having a thin and stooped physique, because I had written the posture theory to explain my own symptoms, and I had that physique. However, my theory evolved from observations that symptoms were related to leaning forward, and I wasn’t fully aware of my own physique until after I wrote the theory and looked at myself sideways in the mirror. I then asked my neighbours for their opinion, and they said that I had a terrible posture, and that when I walked past them and they viewed me from the side my spine was S-shaped. I have since noticed that chest shape and other factors are important. However, many people will have such a physique and not be aware of it, and they will have the symptoms and argue with my assessment of the cause. Furthermore, I have since concluded that there are several different causes and types of chronic fatigue syndrome, which adds to the confusion. Consequently, some people are skeptical of my theory, and I have some extremely hostile critics, who try to argue that I am a fringy kook and that my ideas are nonsense. Nevertheless, the fact remains that some of the world’s top research authorities have described the thin and stooped physique as “typical” of such patients, and The Posture Theory explains cause and effect. |

On a recent tweet from Tom Kindlon (13-10-13) I found a webpage called Health Rising where a woman named Carol Lefelt describes her problems with chronic fatigue.
She reports the likely inheritance of her mothers physique which was a “SKINNY UPPER TORSO” and broad hips which gave her a pear shaped build, and she later adds that she has inherited “osteoporosis” from her “DOWAGER-HUMPED MOTHER” (which means hunchback posture with a forward curvature of the upper spine).
In other words she has the typical thin and stooped physique with a long narrow or flat chest.
She also reports developing the chronic fatigue syndrome and how it impairs her activity and exercise levels etc. i.e. the typical symptoms. See here.

Tight Belts and Tunics
In the nineteenth century it was common practice for some of the soldiers of most armies to create a broad shouldered appearance by tightening their belts to narrow their waist, which would have restricted their capacity for deep breathing, which is required during exertion, such as marching at double quick pace with a heavy, fully laden knapsacks held onto their shoulders by chest straps. Many wore tight military tunics, and some even wore tight military corsets which also restrict the expansion and contraction of the chest during exertion. M.B.See an example of a military tunic here, and an argument about it here.
See also here
A typical Da Costa’s patient
Including the past and present physique, health, and personal history
He was generally aged 30, and previously did clerical work but was currently unemployed, He had a thin build and long chest, was never robust, got frequent sore throats and colds as a child, had his tonsils and appendix out, and was “unable to sit and lie quietly”. He also had a weak stomach, and had his kidneys damaged by Scarlet fever, and there were frequent fluctuations in the color and volume of his urine. “He has always been nervous and easily fatigued”, and he “was never allowed” to take part in competitive sports and has felt inferior physically to others of his own age. He ‘never got over’ his attack of grippe three years ago, and since then has had gradually increasing pain in his heart, shortness of breath, dizziness, faintness and weakness. All of his symptoms are made worse by exertion or nervous strain”. . .the breathlessness “is not true air hunger, but literally a ‘shortness of breath,’ a feeling that deep breath cannot be achieved. The patient usually localizes this sensation in the chest wall itself” . . . “which seems unable to expand normally“, and this produces frequent sighing, which “is not commonly present in patients with organic heart disease”, and is important in making that distinction in diagnosis . . . and “many theories” have been used in the past to explain the cause of the syndrome, and have since been disproven or applied ot “a selected group of cases”. There had been widely varying opinions which may each have a “fragment of truth”. The 1939 author mentioned ten which included “Pressure from clothing”.
Reference: Caugney J.L. Jnr., M.D. (April 1939), Cardiovascular Neurosis; A review. Psychosomatic Medicine,Vol.1 No.3, April 1939
Another reference which describes the typical physique
The constitutional type occurred in children, youth, and early adult life, and most soldier’s who developed it already has the minor syjmjptoms prior to enlistment . This type were generally tall and thin, with long narrow chests which are ’rounded in cross-section’, and forward curvature of the lower spine which pushed the abdomen forward into a ‘bottle-shaped’ appearance, and included visceroptosis with the heart, stomach, and liver etc positioned lower in the torso.
“The next commonest type is of course build. The chest is broad but flat.”
Symptoms: The pulse rate changes when they move from the upright to the reclining position, or in response to fear or other emotional stimulus, and they get palpitations with violent effort “such as the usual exercise test of hopping or forward bending” with the pulse rate taking up to several hours to return to normal. There is soreness in the skin on the left side of the chest in one quarter of cases, and in others there is general sensitivity in parts of the chest, but mainly in one rib space. Giddiness occurs mainly when getting out of bed, or with physical or emotional effort, and tends to become less noticed later in the day. Faintness or sometimes actual fainting occurs with patients reporting from 1 to 100 times, and is brought on by “the cessation of sudden effort, severe coughing attacks, deep breathing, the effort to stool, the sight of blood, a typhoid inoculation,, or a small pox vaccination”. In most cases the patient feels the faint coming on and sits down to avoid falling and injuring themselves. During the faint the pulse may become imperceptible but gradually return to normal after a few seconds or up to five minutes. Dermatographia is the ability to write on the skin where running a fingernail lightly down the skin leaves a red or white line, and according “dermtographia is practically universal”.
Medical tests: “Orthodiography, x-ray, and fluroscopy” have shown “small” hearts which overact and “swings widely” “like a see-saw”. Blood pressure observations correspond to the extreme lability of the entire vascular apparatus”, but cardiograms are normal and there was no evidence of disease of the heart, and it is important to interpret those factors properly so that the patient does not develop cardiophobia (fear of heart disease), as that will not be helpful in treating the problem. The post viral types generally recover, but the ‘constitutional’ types involve “periods of practical recovery and remission”. Reference: Rothschild Marcus A. (April 1930) Neurocirculatory Asthenia, The New York Academy of Medicine, Vol.VI, No.4, p.223-242.(Annual Graduate Fortnight, Functional and Nervous Problems in Medicine and Surgery, October 7 to 19, 1929)
Da Costa’s Syndrome and the medical research literature
“Da Costa’s Syndrome . . . common among solders” . . . Bouts of palpitations, dizziness, chest pain, breathlessness etc . . . “Hard field service was the chief assignable cause in 34.5% of cases . . . as in case 110 after a march of 26 miles in one day . . . ” “Undoubtedly, the waist belt, but particularly the knapsack, may have had something to do with aggravating the trouble, but I could find no proof that they had produced it”. . . .. “The pulse is always greatly and rapidly influenced by position . . . Dizziness was often complained of”. It was increased by stooping (case 44); by exercise (case 57) or by laying on the left side in some cases or on the right side or the back in others. For treatment . . . “Their equipments be such as will not unnecessarily constrict and thus retard or prevent recovery”.
Case 48 enlisted aged 17 with a thin chest of 27 inches, and suffered dizziness, cardiac pain, shortness of breath, and palpitations while on picket duty, and on one occasion while marching when he dropped out and discarded his knapsack and extra clothing, yet still struggled to keep up with the regiment. He was hospitalised and recovered but recommended for the veteran reserve. When examined in civilian practice 8 years later he was a tall, broad chested man who had spent most of the intervening years working in the open air as a mounted soldier. He only had two bouts of palpitations associated with bilious spells, and occasional colds, and otherwise had perfect health with no other symptoms at all, and could run up and down stairs without getting short of breath. Reference: Da Costa J.M. (January 1871), On Irritable Heart, The American Journal of the Medical Sciences p.18-52
Da Costa’s Syndrome . . . “It is concluded that there is some association between left thoracic (chest) pain, and poor diaphragmatic or lower thoracic movement. (The diaphragm doesn’t rise completely when exhaling and the lower chest has poor expansion). A more severe left-sided chest pain can be brought on by “strain of certain muscular attachments involved in such actions as cranking a lorry or lifting a heavy weight”.
Reference: Wood P. (May 24th 1941) Da Costa’s Syndrome, The British Medical Journal, Vol.1, 1941 p.767-772
Da Costa’s syndrome . . . “In some the chest is long and narrow, or flattened and associated with a kyphotic (stooped) curve … slight build … chest wall deformities … (the condition affects) …sedentary town dwellers … commoner in women” . . . “the pulse shows an exaggerated reaction to posture” . . . “there is “breathlessnes” and “suspected – alteration in the character of the blood “acidosis as produced by CO2, or lactic acid) as a causative factor. Fatigue Fatigue was an almost universal complaint.” . . . “these symptoms and signs are largely, in some cases wholly, the exaggerated physiological response to exercise“. . . prompting the name “effort syndrome“. Reference: Wooley C.F. (May 1976) Where are the Diseases of Yesteryear, Circulation p. 749-751.
See more about Da Costa’s syndrome here
See information about the affects of physique and chest shape on the health of animals here
The Posture Theory and Osteopathy evidence & theory
The Australasian Nurses Journal published my essay called The Matter of Framework in June 1980. It took me five years of observing and describing my own symptoms while reading the literature of medicine and anatomy before I could draw that conclusion from evidence which was so obscure that no-one else had been able to recognise it, and no-one else was discussing it seriously. The initial name of that essay was The Posture Theory, so after it was published I wrote summaries of it under it’s original name. A list of those publihed aritcles can be seen here. They were written with the idea that other authors and researchers could investigate and confirm my findings, and other patients could benefit from the change in approach, but very few people have mentioned my name. The following list is a brief sample . . .
January/March 1984, The Posture Theory, Australasian Health and Healing, p.13
April 1984, The Posture Theory Revisited, Natural Health, p. 11
August 1985, Chronic fatigue, A new alternative theory, Natural Health, p.16-17
April 1987, Physical breakdown, The Gully Breeze,
20-3-93 Arataeus, hysteria and hypochondria (a letter about posture and pregnancy and how the enlarging womb compresses the internal anatomy to cause symptoms), The truth – national newspaper,
8-12-1994 – Posture and illness, South Australian Statewide newspaper (a review by the editor)
Winter 1997 – The Posture Theory the physical basis for hypochondria, The Australian Journal of Osteopathy (as reviewed by Alison Linn)
May 1997 – Muscle stress and strain by
Osteopath Andrew Wilson (who used The Posture Theory diagram to illustrate his article). Healthy Options (A New Zealand journal)
See some recent You tube videos on the Osteopathic research into posture and chronic fatigue by Osteopath Dr. Raymond Perring who is looking at how poor posture compresses the lymph vessels as a hypothesis on the cause of symptoms . . .
About The Author
This item was probably started in 2008, with some minor changes since then. e.g. the addition of the photo in March 2012.
The following information was added to this website after several Wikipedia editors asked me to provide details about my own research and publications, and to make it available online so that it would be easy for them to check. My eBook called The Posture Theory is available through here, and a YouTube video of that theory is here.
Before and after my research project (1982-84)Before I did my research the general attitude was that chronic fatigue was not a physical problem, but was all in the patients mind, or was due to laziness, the lack of exercise, or the fear of exercise, and they were being encouraged to run faster and faster each week with the idea that they would regain normal energy levels and normal health, and hence a cure. However all of the patients dropped our of the courses. Added here on 28-9-13 A modern research paper (2010)I knew in 1976, and scientifically proved, in 1982, that the response to exercise in chronic fatigue was abnormal, and described it as a defining feature which distinguished it from normal responses, and other illnesses, and that sooner or later it would become standard and widely accepted knowledge. Added here on 28-9-13 A modern Canadian definitionThis is a quote from an article in the CFIDS Association of America which I read on 28-9-13. “A key difference between these two definitions is that the Canadian definition identifies post-exertional malaise/fatigue (PEM) as a required symptom, whereas the Fukuda definition makes PEM “optional,” as one of eight case-identifying symptoms. Four of those eight symptoms must be present for a case to be considered CFS under the Fukuda research criteria. |
 Max Banfield
Max Banfield
In 1982 the head of the South Australian Institute for Fitness Research and Training invited me to design a program which would solve an international research problem – How do you get scientific data on patients with chronic fatigue, when they all cannot, or will not train.
The principle was to have them exercise within their own limits, and it was successful.
That principles has since been duplicated many times all around the world.
In 1969 I was a gymnastics instructor and was offered three scholarships to do youth leadership training in the Group Work course at the South Australian Institute of Technology. The first was from the National Fitness Council of Australia, N.S.W. HQ. (“responsible for . . . the organisation of training courses in physical education”), which was followed by a South Australian State Government Department of Community Welfare offer of full time study on full salary, and then a Commonwealth Government offer for part time study over four years, which I accepted, and completed.
In 1975 I became interested in fitness and fatigue research, and in 1981 I approached Tony Sedgewick, Head of the S.A. Institute for Fitness Research and Training, which was associated with the University of Adelaide, I discussed the international research problem of not being able to get useful data on fatigue patients, because they either refused to train, or dropped out of the programs too soon to get meaningful results. He asked me to develop a methodology for solving the problem, and a few months later I provided him with a programme design to consider, and the principles were (1) The condition involved different degrees of severity, (2) the patients should train within their own limits, and (3) they should improve at their own rate.
I was then invited to co-ordinate a research study on the subject, which initially involved obtaining a small research grant from the South Australian State Government Department of Recreation of Sport, and establishing a programme committee, I also obtained the co-operation of a medical journalist for the states afternoon newspaper who wrote articles for the purpose of recruiting trainees who had persistent or recurring problems with fatigue. The medical examinations were conducted by two of the institutes research cardiologists.
Over the next two years the IFRT received more than 200 enquiries, and 80 patients were medically assessed, and their exertional capacity was measured using standard scientifically reliable graphs of pulse over load on an ergometric cycle. 9 participants completed training which consisted of light exercise, and walking, or jogging. They were two hourly sessions for two nights per week, for three months or more, and 5 completed 6 months or more.
The results showed (1) those who didn’t train stayed at the same ergometric capacity (2) three improved for 3 months and then leveled out below standard levels, and (3) one improved slowly for the first 3 months, and then significantly improved in the second term. In one group six individuals trained in the same class for three months and their position from first to sixth while walking or jogging around the oval corresponded to their scientifically measured aerobic capacity. A lifestyle questionnaire was also included at the outset, and those who had previously changed and restricted their lifestyle because of their fatigue were found to have low to very low aerobic measurements, and those who did not need to change lifestyle had average to above ergometric results. A general account of the results were reported in the major newspapers in 4 of the 6 Australian states between 1982 and 1983. e.g. See a copy of one of those newspaper reports here. Some years later, when reviewing the results I came to the conclusion that the mixed data was the result of recruiting patients with fatigue, which, in relation to the dual meaning of the word, would bring 3 different groups to the programme (1) those with sleep disorders who were abnormally tired (2) those who had a physical disorder which affected their capacity for exertion, and (3) those who had a mixture of both.
(The research design principles, results, references, charts, and 48 interviews on cause and symptoms can be seen here)
Nowadays (2008) similar programs have been implemented and assessed with several studies showing variable results, where some patients benefit from the programme and others have problems. In the latter case it is probably because they increase their exercise levels at too fast a rate, or exceed their limits and experience the type of symptoms that deter them from continuing. That could be prevented by voluntary participation, with the individual initially walking at a casual pace of their choice, and progressing at their own rate, if and when possible. The condition involves varying degrees of severity from person to person and day to day which requires progress, if any, to be flexible, rather than regulated or expected according to an orderly gradient of improvement, with the person free to choose to stop training, if and when they reach a level of improvement that ceases to benefit from additional training, or to remain at that level as part of a maintenance programme. Other groups of patients, such as those with asthma, arthritis, obesity, or heart disease, may also be limited in their capacity for exertion, but to a different degree, and for different reasons. M.B.
Graded Exercise Therapy, or “GET is one of the most common treatments for CFS” (chronic fatigue syndrome) Another similar method of treatment which relates to keeping within exercise and lifestyle limits is called “pacing” and there are several versions of it based on the general principle of “Self-controlled rest and exercise”.
“Self-controlled rest and exercise, “pacing”: “Pacing” is being advocated by many patients as one of the few really effective means of minimising homeostatic disequilibrium. The principles involve acceptance of the patient’s limitations (by both the patient and any coaches), awareness of the early signals of deterioration e.g. increased cognitive difficulties, pain, clumsiness, muscle weakness, respiratory problems; and stopping exercise/activity before exceeding limitation or “crashing.” A good rule of thumb is to never exert more than 70% of capacity. An understanding nurse, doctor or physical therapist may be of help.”
Reference 1 : Hurst, J.W.; R.B.Logue, R.C.Schlant, N.K.Wenber (1974). The Heart 3rd. edition. New York: McGraw Hill Book Co.,, 1552-1555 – The authors of this paper stated “attempts by Cohen and his associates to alter these abnormalities by physical training were unsuccessful since the patients could not or would not follow the prescribed training programme.” and commented that previous studies of a small number of patients by Holmgren in 1959 and Levander-Lindgren in 1964 has shown that training programs had shown some benefits. It was the comment that these patients “would not or could not train” that prompted me to design a programme that patients “could and would train” if they were instructed to train within their own limits.
A scan from J.W.Hurst’s 1974 book where he reports that Cohen and his associates were unable to get their chronic fatigue patients to exercise
Reference 2: Wikipedia, Chronic fatigue syndrome, history of edits, 18:38, 27-9-07, 5.1.2.
>See also Wikipedia “Chronic Fatigue Syndrome 2.3, & 2,4, & 5.1.2” (30-12-07), and click on the history tab and scroll down to the date 30-12-07, and the end of 5.1.2 to see the “pacing” paragraph, which was deleted from the wikipedia CFS page at 11:22 on 5-1-08. Note that the links will now only lead to the current page on CFS where the pacing details have been removed.
Wikipedia (1-1-08) – CFS ref.. 178. The “Gibson Report” Report of the Group on Scientific Research into Myalgic Encephalomyelitis (2006)
Wikipedia (1-1-08) – CFS ref. 188. Peter D White, Michael C Sharpe, Trudie Chalder, Julia C DeCesare, Rebecca Walwyn for the PACE trial group (2007). “Protocol for the PACE trial: A randomised controlled trial of adaptive pacing, cognitive behaviour therapy, and graded exercise as supplements to standardised specialist medical care versus standardised specialist medical care alone for patients with the chronic fatigue syndrome/myalgic encephalomyelitis or encephalopathy.”. BMC Neurology 7:6. DOI 10.1186/1471-2377-7-6.
See also: Better Connect Channel (20-1-08) – Chronic fatigue syndrome and Exercise:: Health and medical information for consumers, quality assured by the Victorian government (Australia).
see also: Harrison’s Principles of Internal Medicine 17th edition. New York U.S.A.: McGraw-Hill Companies Inc., 2703=2704. The text of this summary links the former term “effort syndrome” to the modern condition of “chronic fatigue syndrome” and refers to graded exercise regimes which have “proven” effective in relieving symptoms and improving exercise tolerance.
See also; The Disease of a Thousand Names Compiled on-line by medical consumer Melissa Kaplan, last updated April 19, 2007.
“The cause of CFS is unknown, although a large number of causes have been proposed, and several proposed causes have very vocal and partisan advocates. In a basic overview of CFS for health professionals, the CDC states that “After more than 3,000 research studies, there is now abundant scientific evidence that CFS is a real physiological illness.“[50] The cause of CFS may be different for different patients, but if so, the various causes may result in a common clinical outcome.”
Reference: Wikipedia, Chronic fatigue syndrome, 10:21, 8-1-07, 3. and, ref: (50) CDC – CFS Basic Overview (PDF file, 31 KB), U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. See here and here.
Chronic fatigue syndrome includes a large range of ailments which involve the symptom of fatigue as one of the main features. Throughout the history of these conditions there have been differences of opinions and controversies about cause and nature, between doctors from one specialty to another, and from those who believe it is “all in the mind” to those who think it is physical, and from doctor to patient, and from one individual or group of patients to another. It appears as if different causes are being argued about as if they relate to the same condition, so in order to clarify the difference between anxiety, sleep, or exertional disorders, for example, it is necessary to clearly, accurately, and precisely identify each of the many sub-types of which Da Costa’s syndrome is one of the exertional disorders, where the patients do not necessarily have a fear of exertion or heart disease, and they don’t necessarily have agoraphobia or panic attacks, and are not necessarily depressed or having nightmares, and may or may not have recollection of previous exposure to viral infections or toxic chemicals, etc. M.B.
Leadership by example
When I studied leadership I came to the conclusion that I had one natural aptitude to “lead by example”. I am not a dictator.
In relation to chronic fatigue I have studied the problem and know how to manage the symptoms, but I don’t expect anyone to believe me if they don’t want to. It is up to each person to decide if my methods help them or not.
The History of theories about the supposed fear of exercise, and how I changed the course of medical research.
1919 Sir Thomas Lewis was studying fatigue in soldiers which had been called Da Costa’s syndrome, and Soldier’s Heart, and he renamed it the “Effort Syndrome” because of the relationship of the symptoms to physical exertion.
1939 J.L. Caughey reviewed the relevant medical literature of that time and gives a typical example of the patient where “He ‘was never allowed’ to take part in competitive sports and has felt inferior physically to others of his own age“.
1956 Paul Wood O.B.E. Britain’s top authority on that topic attributed the symptoms to anxiety, and concluded that the abnormal response to exercise was due to the fear of the normal symptoms. He described it as a psychiatric condition which usually involved an anxiety state where, in many cases, the adult had been a timid child “far too dependent of maternal protection. At school, kindly doctors and soft mothers protected them from the hazards of football, swimming, and the gymnasium“. See my report here.
1974 J.W. Hurst wrote a reference book for cardiologists which included this topic and these words . . . “the patients could not or would not follow the prescribed training programme.
1975 I began treating my own ailment with rest and mild exercise at the S.A.Institute for Fitness Research and Training, and later, when I read research papers and books which attributed the symptoms to the fear of exercise I knew they were wrong, and began explaining the physical nature of the problems and how they differed from the normal response to exertion.
1982 I explained my ideas to Tony Sedgewick who was the head of that organisation and he immediately recognised their importance, and when his own professional research cardiologists were too busy on other studies he asked me to design and co-ordinate it. The project was successful through three consecutive training periods of 12 weeks each, and proved that the problem was physical, and was not due to the fear of exercise. The principles included training within limits, and stopping if there were any problems before resuming again.
1987 Simon Wessely began studying chronic fatigue and using the same principles which he called Graded Exercise Therapy.
2012 Simon Wessely was given the John Maddox Prize for courage in science in relation to his study of Graded Exercise Therapy for the Chronic Fatigue Syndrome.
December 2012 Simon Wessely was knighted for his contributions to medicine in relation to chronic fatigue treatment for civilians and Soldier’s.
The Graded exercise program of Sir Thomas Lewis in 1919
As you can appreciate, in 1975 I was experiencing problems with exertion which was not responding to any form of medication or treatment, so I had to determine how to treat the problems for myself. I did so by trial and error, and 7 years later was asked to design a research project where I established that other patients with fatigue could also benefit.
However many more years went by when I became interested in the history of the subject, and I found a book by Sir Thomas Lewis which had been published in 1919. At that time the condition had many labels such as Da Costa’s syndrome and he renamed it the “Effort Syndrome”.
Given that nobody had ever told me about such things I was surprised to find that he had used Graded exercises in his research.
His main objective was to determine the fatigued soldier’s capacity for duty, and to try and return them to full service.
The instructors were chosen from those who were experienced in normal army drill, and applied exactly the same exercises.
They were told to start with light exercise for 15 minutes, and in due course to increase the number and strenuousness of the exercises, and to increase the time to 30 minutes. In the next levels they included slow marches for 1-2 miles in the afternoon, and eventually longer marches of 4-5 miles at ordinary pace.
The instructors were required to report instances where the soldier’s had difficulty with the exercises and they were then sent for medical assessment. Otherwise the program would continue to the next level. Nevertheless, some officers decided to increase the levels automatically, and assess the complaints as they occurred.
Some of the soldiers’ were unable to exercise, or had problems with light exercise and were discharged from duty. Others who had a higher capacity were recommended for light duties, and others with full capacity returned to full military duties.
In his concluding comments he wrote these words . . . “In the majority of the patients progress occurs to a point and there is no further improvement, health remaining impaired or imperfectly restored”.
My method of exercise which I developed independently in 1976 has some similarities
I began with light exercises which meant no push ups or heavy lifting. I started with slow walking for short distances and very gradually increased the pace and distance, as it became possible to do so. If I had any problems I slowed down or stopped and started again, and kept training for the same period of time as others in the exercise program. For example, if everyone else was jogging or running for 30 minutes, then I would be walking or slowly jogging intermittently for 30 minutes. If they walked a mile in 8 minutes, then I would walk and intermittently jog slowly until I covered the same distance. I kept doing that for almost a year, up to six times a week, before I injured my knee and stopped.
My aerobic capacity was scientifically measured at the start and after the first 12 weeks, and again some time later. It increased significantly in the first period, but then, despite training at improved levels, for longer distances, more often per week, my aerobic capacity remained the same.
When I designed the research project 7 years later I advised the instructor to put people with fatigue in their own group where each individual was required to exercise at their own level regardless of what others were doing.
Since then it has been possible to train some patients with chronic fatigue syndrome in a reliable and consistent way by using those principles, and they can be seen in programs called PACING and Graded Exercise Therapy.
There are a number of other differences which I may discuss later.
Simon Wessely is “simply” WRONG
In November 2012 Simon Wessely was given the John Maddox Prize for courage in science related to his research into chronic fatigue syndrome and exercise, and soon after that was Knighted.
He argues (or is telling lies) when he says that chronic fatigue is due to “inappropriate illness beliefs“, “pervasive inactivity” (lack of exercise), and that there are “no physical signs of disease“, and “no pathology causing the patients symptoms“, and that the patients are just “hypervigilant” (excessively concerned) about “normal bodily sensations“.
However, I have CFS but as a teenager I played some sort of sport every day of the week, and four hours of gymnastics from 7 -11p.m. was just the first day of a 7 day week, so Wessely’s claims about inactivity being the cause is not only wrong, it is utterly ridiculous.
I was involved in gymnastics for 10 years, and only had one injury, and occasionally when running at full speed, and missing the end of the springboard, and going head first into a wooden horse, my policy was – do it again immediately, otherwise you might never do it again. I also often fell off the five foot high wooden horse, or somersaulted at the wrong angle and missed the mat, and would just get up and do it all again, often several times a night, especially when practicing the dangerous stunts. The suggestion that I was “hypervigilant” or overly concerned about trivial cuts, bruises, or disease, is again, ridiculous.
When I read the medical literature I found an enormous amount of evidence of physical causes, and when I added it to Wikipedia, two editors deleted it. See here. It was obvious to me that they want the Wikipedia readers to believe that it is a mental disorder, and as is typical of deceitful individuals, they don’t want the facts to get in the way of their stories.
Wessely’s comments can be seen in the link below, followed by my report on CFS, sport, and exercise.
@AzurebluS This is why I tweeted Simon Wessely..*grits teeth* x pic.twitter.com/SRsWanhKpp
— Fiona Craig (@FionaCraig94) September 11, 2013
My interest in sport many years before developing Da Costa’s syndrome
This item was added in April 2012. See an earlier item here
 I did this summersault when I was about 17 years old at an annual demonstration of the gymnastics club in front of an audience of over 100 people.
I did this summersault when I was about 17 years old at an annual demonstration of the gymnastics club in front of an audience of over 100 people.
The unicycle was about 9 foot six high, and my feet were about two feet higher when I rotated through the summersault.The ceiling of a 2 story building is visible.
My main interest as a teenager was gymnastics, in which I would attend the gym up to three or more times a week, often for up to five hours at a time. On other days, and on weekends, my other interests included athletics, sport and swimming. I participated in one mile, and cross country races, and could easily swim from jetty to shore, or across rivers.
However, one of the most popular ideas about the cause of Da Costa’s syndrome is that such individuals did not play sport when they were young because the didn’t want to, or their parents wouldn’t let them do anything where they might get hurt. Consequently, it was argued that the person never learnt the difference between the normal symptoms of exercise, and the symptoms of lung or heart disease.
It was suggested that when they exercised, and the normal symptoms occurred, they thought it was due to disease, and the anxiety made the symptoms worse so they avoided exercise. Some have since put that in the psychiatric context by calling it “avoidance behaviour“?, but that label could be equally applied to someone sensible who looks both way before crossing the road to avoid being run over by cars, buses and trucks.
It was then thought that they became unfit because of the lack of exercise, and hence ‘exercise intolerant’, and therefore experienced more severe symptoms in relation to exertion than a ‘fit’ person, so they continued to avoid exercise.
Therefore it was said, that all you have to do is convince them that their symptoms are normal, and to get them to exercise at gradually increasing stages to overcome their fear, and return to normal levels of activity.
One of the exponents of such ideas was Paul Wood O.B.E., who was very influential, and changed the general attitude towards anxiety theories after the 1950’s, and those ideas are still very popular among many researchers today.
However, while such ideas sound ‘plausible’ and may have a grain of truth in some cases, and while it is sensible not to mention anything which would make such individuals worry, it nevertheless, has to be said that such problems are “exercise phobias”, or “cardiophobias”, and not Da Costa’s syndrome.
In fact, many people who played sport when they were young, including myself, had to give it up because of the abnormal response to exertion which occurs in Da Costa’s syndrome.
I had often ran myself to exhaustion from one end of a sports field to another, being pursued by other players, or when overtaking dozens of other runners to beat them at the closing stages of a cross country race, but the ordinary symptoms of such normal exercise are not even remotely the same as those of Da Costa’s syndrome.
In fact the symptoms of Da Costa’s syndrome are physically based, and consistent in their nature, and are different from the symptoms of normal or vigorous exertion, and are are also different from the symptoms of fear, anxiety, or any other emotion. The confusion relates to the fact that they all involve factors which influence heart rate, blood pressure, breathing pattern, chest pains, faintness, and fatigue. See my reports here and here.
Notes of the picture above
One of the women in the back row looks worried about the possibility that I might fall in her direction.
The man standing at the back on the left was my father. He was a keen sportsman himself and played table tennis, snooker, darts, and night cricket at the local branch of the Returned Servicemens League, and later became it’s president.
He was treasurer of the gym club.
The certificates and trophies were presented to the students by the local member of Parliament.
One of the references which is very typical the ideas about psychological cause, and psychological “conditioning” is T. Troosters et. al. (1999) Physical performance of patients with numerous psychosomatic complaints suggestive of hyperventilation. European Respiratory Journal, 14, p.1314-1319. (The author traces this problem back to Da Costa of 1871, and Lewis 1918, whose research papers he used in his reference list as number 1, and 2).
This is a quote from his conclusion . . .
“It seems therefore, that the sequence of events responsible
for symptoms and breathing abnormalities during
exercise in this group of patients is as follows. Firstly, a
psychological conditioning process generated by, or linked
to exercise, might be the origin of the many symptoms, i.e.
the high anxiety level and a peculiar breathing pattern. The
symptoms, when marked, result in a tendency to hyperventilate
during and following exercise, with production of
new symptoms (paresthesias, dizziness). The learned response
is then reinforced by every new trial to exercise.
Finally, the occurrence of symptoms with the slightest
exertion leads to a reduction of physical activity and an
ensuing deterioration of exercise tolerance.” See here
A second reference to such ideas can be seen in Paul Wood’s book of 1956, Diseases of the Heart and Circulation. 2nd. edition, Eyre & Spottiswoode, London, p.937, and 947. He convinced the majority of researchers that it was an anxiety disorder, and that is still the prevailing opinion today. See also the opinion of a Wikipedia editor praising his credibility here.
He attributes the symptoms to a variety of “fears”. This is a quote from his book where he discusses the type of adult who develops the ailment . . .
“They are timid children, far too dependent upon maternal protection. At school kindly doctors and soft mothers protected them from the hazards of football, swimming, and the gymnasium. . . . Fear of football, and fear of swimming are common in childhood“.
See another website which reports on an individual with chronic fatigue who had previously led a very active life here.
From Anxiety State and Psychotherapy 1939-1974 The following words are a quote from a review of the literature of internal medicine by J.L.Caughey Jr. in 1939 “The typical patient with the ‘effort syndrome‘ was “”never allowed’ to take part in competitive sports” and has felt inferior physically to others of his own age”. . . “They never learned to keep on when the going was hard” . . . during the exercise test . . . “the response is no more dependent on the amount of exertion as it is than on the emotional reaction he has, the fear that he has that the test will injure seriously his already weakened heart” Reference: Caughey J.L. Jr. M.D.(April 1939) Cardiovascular Neuroses: A Review. Psychosomatic MedicineVol.1, No.2, p.311-324. see my full report here The following quote is a photocopy of a section of a book by Paul Wood in 1956
| to the Chronic Fatigue Syndrome and Graded Exercise Therapy 1975-2013
It contains a chapter on this topic, and on page 937 he states “one may speak of Da Costa’s syndrome to cover all previous nomenclature”. In other words it is the name covering this topic which has symptoms of chest pain, breathlessness and fatigue where there is no evidence of heart disease. I have scanned two paragraphs from his comments of page 943, and posted them on the left. He was a top authority on the subject and his opinion was the most widely accepted up until 1975 when I started studying and writing about it, but I didn’t find his book until much later. He believed that the symptoms of Da Costa’s syndrome were the same as those of exercise phobia, and cardio phobia etc. but I have proof that they are different. See how I prevented the harmful effects of exercise, and why I advised other CFS patients how to do it here. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
I proved that chronic fatigue syndrome was NOT due to a lack of exercise in 1976, but some researchers still argue that it is????
On 17-10-13 Simon McGrath provided a Twitter link to the Phoenix Rising website review of the following research paper . . . Lucy V Clark and Peter D White 2005, “The role of deconditioning and therapeutic exercise in chronic fatigue syndrome (CFS), Journal of Mental Health 2005, Vol. 14, No. 3 , Pages 237-252 (doi:10.1080/09638230500136308” here.
Note that deconditioning refers to the idea that a physically fit person is in good physical condition and that the lack of exercise causes a person to become unfit, or “deconditioned”. Some modern researchers believe that the ready fatigueability of patients who have the chronic fatigue syndrome is due to the lack or fear of exercie, and base exercise treatment on the idea that improving fitness will reverse the process.
I was the first
| I was the first person to invent the method of using exercise in the gradual way , within limits, in 1976, to treat my own illness, and scientifically proved it’s effectiveness in a 1982-3 project. The theory was that the problem was due to a physically based impaired capacity for exertion, and that it would be possible to improve if the person stayed withing their limits (nobody had ever thought of that idea before). | However, in the review below the author isn’t mentioning my name, and is obviously referring to someone else who has copied my idea, and who they say was the first person to develop that method, and presented a different “reason”, namely, that it is due to a lack of exercise., and therefore that it can be reversed by exercise. |
 You can see clearly that I was not lacking in exercise or “exhibiting exercise avoidance behaviour” before developing the chronic fatigue syndrome
You can see clearly that I was not lacking in exercise or “exhibiting exercise avoidance behaviour” before developing the chronic fatigue syndrome
The aims of the report were . . . “To review the literature relating to the role of deconditioning in perpetuating CFS and the literature relating to the role of graded exercise therapy as a treatment of CFS” (end of quote)
This is a quote from that review . .
“Therapeutic exercise programmes were first designed for patients with CFS on the basis of reversing physical deconditioning. However, they are also a behavioural graded exposure treatment thought to work by habituating the patient to the stimulus of exercise which has caused the conditioned response of fatigue and malaise. (end of quote).
This is another quote . . .
“Background: Patients with chronic fatigue syndrome (CFS) complain of tiredness or exhaustion, which is made worse by physical exertion.
This results in their avoidance of exercise, which may lead to physical deconditioning.
We do not know whether this deconditioning maintains the illness or is a consequence.
Graded exercise therapy aims to reverse this cycle of inactivity and deconditioning, and to subsequently reduce the fatigue and disability associated with CFS” (end of quote)
This is another quote . . .
“If a patient develops symptoms as a response to increased activity, they should keep exercising at that level, rather than either stop or increase the intensity/duration. As the body adapts and symptoms subside, they should then be encouraged to increase by an incremental point again, mutually agreed between therapist and patient.” (end of quotes).
This is third quote from that report
“Treatment is based upon the theory that exercise avoidance perpetuates symptoms through deconditioning, a reconditioned response, and changes in interoception. Modifying avoidant behaviour breaks the vicious circle of fatigue and disability; physiological consequences are reversed, promoting recovery.
Another quote . . .
“In summary, patients with CFS reduce their participation in physical activity, which could exacerbate or perpetuate their fatigue. The possible mechanisms are: directly through reduced physical strength and cardiovascular deconditioning, or indirectly through the physiological consequences of inactivity such as autonomic nervous system changes, hypothalamic-pituitary – adrenal (HPA) axis down-regulation (leading to low cortisol concentrations), or through changes in central nervous system interoception. Such impairments lead to symptoms at a lower level of physical activity. The inability to function at previous levels may lead to frustration, low mood and a lack of motivation and lethargy. A vicious circle of increased exercise avoidance and symptoms occurs, which serves to perpetuate fatigue, and therefore CFS. Edwards (1986) was the first to illustrate how inactivity, brought about by fatigue, can itself exacerbate and perpetuate fatigue” (end of quotes)
You can see that the modern researchers are talking about my methods of treating chronic fatigue with exercise, but they still have the mistaken belief that it is due to the fear or lack of exercise. I proved that idea was wrong when I decided to treat my own ailment with exercise by joining a class at the South Australian Institute for Fitness Research and Training in 1976. Nobody told me to do that. It was my idea, and I had to invent a way of making it possible.
Nobody told me that I was supposed to be afraid of exercise???
Notes for the picture on the right
Nobody, not even my doctors, noticed something which is evident in the photo on the right, and would not notice now, unless I mention it.
Many years after developing The Posture Theory I looked back on some old photos, and in this one my right shoulder is much lower, and more rounded than the left.
It is an indication of scoliosis(sideways curvature of the spine), and according to my theory it was the cause of occasional sharp stabbing pains in the lower left side of my chest.
I can also recall that my tailor put padding in the right shoulder of my coats to make the shoulders look even.
That symptom was evident long before I developed the fatigue due to forward curvature of my upper spine, called kyphosis.

Nobody told me that I was supposed to be afraid of exercise when I was young?
My skin/fat ratio was later measured at the fitness research institute, and found to be the same as that of an Olympic athlete.
Because of my experience with sport, I was aware that exercise was excellent for health, but because of Da Costa’s syndrome I had to give it all up. However, I spent the next five years trying to determine the cause of that ailment, and was eventually able to identify a subtle, but definite relationship between the various symptoms and poor posture, and develop methods of relieving them, and ultimately wrote The Posture Theory. In the meantime I wanted to return to my former activities, and I thought that I might be able to do that if I did very mild exercise, and gradually regained my former fitness levels.
I saw an article in a newspaper about an organisation which was conducting medical research into the relationship between illnesses and fitness, so I made some enquiries, and enrolled. After undergoing some medical and fitness tests I began a three month course of training.
There weren’t any courses for people with chronic fatigue, so I joined a general class which included healthy people, and those with lung diseases, asthma, and arthritis etc.
I was walking and slowly jogging, and coming last in the exercise sessions, but managed to complete the course and have my fitness level retested. I then continued for another 3 months, and then a third, but after a couple of months passed I injured my knee cartilage and had to stop. Nevertheless I had established that I had abnormally low fitness, and that it improved with training, but then plateaud and did not return to normal regardless of how many hours, or how many times per week I trained.
I continued to read medical books and research papers to find or develop some methods of improving my health when I found a statement which said it was not possible to get research data about this type of ailment because “these patients could not or would not train.” Other article referred to the patients being too lazy to train, or afraid of exercise, or didn’t want to get better. etc.
I later met a friend of mine who knew the head of the fitness research institute, and recommended that I discuss my ideas with him, so I did, and, during that discussion I told him about the problem that overseas researchers were having with getting scientific data, and explained to him that if I could train, then so could other people with the same ailment, if they did it my way.
He agreed, and then he asked me to design a research programme. The medical staff were too busy on other studies, so he eventually asked me to organise and co-ordinate the programme myself.
It consisted of twice weekly classes of mild aerobic exercise, and walking or jogging within their own limits, and improving at their own rate, and medical and fitness tests at three monthly intervals. It continued successfully for about a year, while I was there, and for some time after.
During that time I was able to establish that it was possible to get some of those patients to exercise, and that they did have abnormally low fitness levels, and that some improved, and some didn’t, and it was due to physical, rather than mental factors. In particular that the poor level of fitness was not due to the fear of exercise, or the lack of exercise, and the tiredness and fatigue was not imaginary, and not just normal tiredness.
Most notably the fitness levels of some of those patients was below the level that is seen in people who do sedentary work, and don’t play sport, and who don’t do any exercise at all. In other words it is not possible to simply attribute the ailment to a lack of exercise. See more details about that research program here.
See more details about my response to exercise before and after developing CFS here.
See more information about my experience surviving many other illnesses here.
The medical ideas of 1975
When I was consulting my doctor in 1975 he had sent me to various medical tests but was unable to diagnose my health problems, or explain the cause, or treat any of the symptoms effectively. He had previously prescribed numerous medications, and at that time I was taking one 500mg capsule of a drug called Sodium Amytal. When he increased the dosage to 750mg I decided to stop taking pills and begin studying medicine to find the cause myself. There were many symptoms, where the main ones were chest pains, palpitations, breathlessness, faintness, fatigue, and abdominal pain. The only fact that I knew at that stage was that they were made worse by leaning toward a desk all day. However,I didn’t know how that could be causing symptoms because I knew absolutely nothing about anatomy or physiology.
My ideas from 1975 onwards
Within a few years I was able to observe the details from my own experience and identify that poor posture was the cause of most if not all of those symptoms, and later that sideways curvature of the spine had an influence, as well as chest shape, where people with broad and deep chests would be unlikely to have the symptoms, and those with long, narrow, flat or receding chests would be more likely to develop the problem. I also later established that similar problems affected nineteenth century women who compressed their chest and abdomen with tight waisted whalebone corsets, and pregnant women whose internal anatomy was compressed as the enlarging womb gradually rose in the abdomen.
I had developed the idea that the faintness was due to the long term affects of postural compression of the air in the chest which impeded the flow of blood between the feet and the brain, and that the chronic fatigue was due to the fact that such repeated pressure strained and damaged the blood vessels below the chest, to produce weak circulation. I also developed, and reviewed other ideas about displacement of the internal anatomy, or visceroptosis being a cause.
I had also observed, and later scientifically proved that the problems with exercise were related to a chronically reduced aerobic capacity, and that the symptoms could be significantly prevented by exercising within individual limits, and extended that idea to include modifying lifestyle to avoid hurrying and worrying, and get more rest, more frequently than healthy people.
The medical theories up until 1975
Portrait of a Da Costa’s syndrome patient showing the typical thin and stooped physique (from a book published in 1956)
See more details here.
Nowadays, I can look back at that experience, and I have acquired a knowledge of the history of medicine, and I can report that in1975 the medical literature of the 1950’s and earlier had included some suggestions that poor posture may have been the cause, but nobody had pursued the idea, and they had been abandoned in favor of the anxiety theories. Similarly, in the early twentieth century the relation between exercise and symptoms had been reported, and graduated exercise programs had been recommended as a treatment. However those programs lost their popularity largely because of negative results where patients would have dropped out of the training when they went beyond their own limits. The general attitude was that the patients could not or would not train, with the implication that they were too lazy, or didn’t want to get better, or were easily discouraged by effort and adversity, or that the symptoms were due to a fear of exercise, the fear of sport, the fear of heart disease or death, and the fear of people, or the fear of everything (agoraphobia). It was also thought that they were afraid of the normal symptoms of emotion and exercise and it was observed that many of the patients were anxious or depressed so, in 1975, the only treatments available were medications to dampen down the symptoms, and psychotherapy for anxiety or depression.
Wikipedia 2007 – 2012
While I was involved in Wikpedia between 2007 and early 2009, I added some of my own ideas to a page about Da Costa’s syndrome and two arrogant and ill-mannered editors described me as a worthless, non-notable fringy kook whose contributions were nonsense, and they argued that the information must come from medical journals and be based on the formal and brief definitions found in dictionaries. Amongst their rather arrogant and offensive statements they suggested that “i meant well” and that I had a “noble” cause, and that I “believed” that my own ideas had practically saved my own life, and that I was “trying to help other people” with my own ideas about “how the body worked” but it was not “appropriate” for Wikipedia. See on of my reports of their
They deleted all of the scientific evidence and proof of physical cause, and all independent scientific evidence which verified my ideas, and replaced it with descriptions of anxiety and imaginary disorders, and mental illnesses. However, they did not recommend psychotherapy, but kept my description of the best way of treating the symptoms which were based entirely on my theory about posture, and my research about exercise.
I recommended improving posture, wearing loose garments, exercising within limits, modifying lifestyle, avoiding stooping, and standing up slowly when necessary to avoid faintness.
They managed to get me banned in January 2009. but my treatment recommendations are the only ones which are still in the article more than three years later, in April 2012, because none of the other editors has had any reason to dispute any word of it. However, my two critics obviously resent the fact that I developed the ideas, and don’t want the public to know, so they haven’t mentioned my name or acknowledged me as the real source of the best information in the world today – 2012.
See the current treatment section here, and how they tried to delete all of my contributions and all information about my theory here, and one of my reports on how they defamed my character here, and examples of their offensive and ill-mannered behaviour here, and their ill-mannered response to me here.
The Arguments
My theory – Posture “is” one of the causes
When I wrote The Posture Theory it was a way of explaining the cause of my own symptoms largely based on my own observations, but at some stage I came across a portrait of the physique of the typical patient, which was exactly the same as my own, and confirmed my conclusions. However, I also set up and attended other groups of people with the same ailment and noticed that they didn’t all have stooped spines, so ultimately I came to the conclusion that such a physique “disposed” to the problem, or made it more likely” to affect those individuals, and that it was “part” of the cause in some cases, and possibly the “main“, or “only” cause in others, but that there were also other possibilities. In other words, the fact that my physique is exactly the same as the typical physique described by some of the top researchers in the world is more than just a coincidence.
Critics who say it can’t be the cause because some patients have good posture
Some people are simpletons who can’t actually think carefully enough to solve problems themselves,. They argue that if the ailment can effect people with good posture, then it is “nonsense” to say that poor posture is the cause. They are like the people who argue that cigarette smoking can’t be the cause of lung cancer because their uncle never smoked and died of lung cancer at the age of 40. However they don’t take into account that other factors such as industrial air pollution can cause the same problem. Critics who say it is nonsense because it is not consistent with “modern” opinion
The other main argument as presented by two Wikipedia editors was that it wasn’t consistent with “modern” ideas, and was therefore nonsense. However many of the ideas which were considered “modern” in the nineteenth century have since been proven wrong. Furthermore, as recently as the 1980’s it was popular to believe that nothing could live in stomach acid, and that it was therefore impossible for stomach ulcers to be caused by microbes, and must be psychosomatic. However, it has since been found that some microbes are “acid resistant” and that the cause is microbial, and curable by anti-biotics. In other words, just because an “opinion” is “modern” and widely accepted, does not mean that all other ideas are wrong.
| Search Engine Submission – AddMe |
|
|
McGraw Hill Education |