Abdominal Pain
Chronic and undetectable types
including Sliding Hernia, Esophageal Achalasia, Heartburn, Reflux, GERD, Indigestion, Irritable Bowel Syndrome, and Unexplained Pain ©
TWAM phenomena & Tracpad
First, a note about my copyright, and intellectual property thieves
I spent 23 years trying to relieve recurring abdominal pain before I developed an effective method of treating it by standing in front of a computer instead of sitting at a desk.
Since then the people who argued that it was “all in the mind” and caused by the psychological stress of sedentary work, are reading my descriptions of how I did it, and stealing my ideas in a few minutes, and claiming that they thought of the physical cause.
Other people are reading their “copies”, in the belief that they were the authors, and broadcasting or recommending, or teaching the method around the world, with the result that no-one is giving me the credit for being the person who helped them to prevent or overcome that type of severe pain for the first time in history.
The public should show me respect for solving a problem that no-one else could solve, and make sure that those copyright thieves don’t get away with the crime of stealing my intellectual property.
Chronic abdominal pain is not “all in the mind”
The major causes are poor posture and tight waisted garments
The compression of internal organs by tight corsets

Tight belts have the same effect
While I was developing The Posture Theory I concluded that throughout history the major cause of chronic abdominal pain was poor posture and tight waisted belts, girdles, and corsets which compress the stomach and bowel and push them permanently out of their normal position in the belly so that the normal smooth curves in those hollow and tubular structures become sharp angled bends. Those sharper bends are prone to kinking and blockage which causes pain and bloating.
The most obvious recommendation for prevention and treatment is to improve posture and not wear tight waisted clothing.
However, the natural healthy and attractive waist is narrow, so when people gain weight and begin to look unattractive they tend to artificially hide or reduce that problem by wearing something to reduce it’s size, and look attractive again. Hence, for example, nineteenth century women took on the practice of wearing extremely tight corsets, in massive numbers, and suffered the most horrendous types of abdominal deformities, diseases, and pain in human history.
However, the pain does not occur immediately after putting on the corset, so most wearers did not notice that it was the cause of their chronic illnesses, but, in fact, it was the cause. When corsets went out of fashion in the early twentieth century the horrendous cases of abdominal disease declined in incidence and were replaced by less severe forms of the same ailments.
Nowadays many people have poor posture, and still try to narrow their waist by wearing tight belts or girdles, and they get chronic abdominal pain without noticing the link between cause and effect.
Apart from treating those ailments by making permanent changes to posture and clothing, the high fibre diet is also useful as a treatment because it produces softer digestive material which flows more easily through the sharper bends in the tubular structures of the abdomen.
More information on corsets and health can be seen here.
Other causes of undetectable abdominal pain are discussed on this page below..
Causes of Undetectable Abdominal Pain © 9-4-11
This section is part of The Posture Theory which explains what I have determined to be the causes of chronic abdominal pains which generally don’t show up on x-rays and are not evident by the various medical tests. I also explain the methods which I have developed to prevent, relieve, minimise, or manage the problems and why they are effective.
There are many causes of chronic abdominal pain such as . . .
1. Injuries to the abdominal muscles or abdominal wall which are not all visible on x-rays.
2. Sliding hernias where part of the stomach slides up and down through the hole in the diaphragm, which can’t be detected unless it is in the chest at the time the x-ray is taken.
3.Tenderness of the inner lining of the stomach and esophagus which are not evident on x-rays or gastroscopy, but are easily aggravated by such things as acidic foods such as oranges etc.
4. Visceroptosis, in which the abdominal organs have been permanently pushed six inches or more below their normal positions by such things as poor posture. Some people have minor displacements with severe pain, but others have severe displacements with no symptoms, so the problem may be evident on x-rays but not be considered or diagnosed as a cause because of the uncertainty of the relevance. The difference may be due to the fact that people with poor posture will be repeatedly compressing the displaced anatomy, but those with good posture won’t.
Treatment of Undetectable Abdominal Pain
If nothing else has helped relieve your pain then you can try the following methods.
However, it is generally necessary to try these things for several weeks to see if there is any benefit.
1. Improving posture will take the weight of the head, shoulders and chest off the diaphragm muscle which divides the chest and abdomen, and will make it less likely for the stomach to pass through the opening between them. Methods for improving posture include the Alexander technique, or Yoga etc.
2. Don’t wear tight waisted garments such as tight waisted corsets, belts, or underwear with tight elastic waistbands which tend to press on, and irritate the internal anatomy, and push the stomach etc upwards and against, and sometimes through the small hole between the abdomen and chest.
3. Don’t bend at the waist (a) if it is necessary to bend then keep the back straight and bend at the hips.
(b) If writing while sitting at a desk is associated with the pain, then try standing at the computer and typing with the keyboard at elbow height and the screen at eye height so that bending isn’t necessary.
(c) If the pain has been aggravated by bending, then lay on your back in a recliner chair for a few minutes or hours until the worst of the pain has subsided. Having the head elevated, with some padding under the lower arch of the back, and the knees slightly bent while reclining may provide some additional effect.
(d) If the pain occurs during sleep, then try sleeping with the head and shoulders elevated and the knees bent. Each of those positions takes reduces the amount of pressure pushing the stomach against the hole between the chest and abdomen.
(e) If the pain is aggravated by stretching upwards or sideways with your arms, then move position so that you don’t need to stretch, or avoid that type of activity.
4. Don’t eat foods that are highly acidic such as oranges or lemons or their juices
5. Don’t eat foods that have blood thinning effects such as raw onion or garlic, and herbs such as ginkgo, or drugs such as aspirin which may aggravate stomach wall sensitivities or increase the bleeding of ulcers.
6. Drinking a small amount of milk can relieve some types of abdominal pain because it puts a thin protective coat on the sore spots in the foodpipe or stomach, and prevents the acid from having direct contact with them
6. Don’t eat foods that have been cooked in strong spices which can also aggravate stomach pain.
7. If constipation is a problem include high fibre foods in your diet. For example, try eating two apples a day for two weeks and see if there is any benefit.
The reasons for the treatment types
1. In the nineteenth century women who wore tight waisted corsets had the most horrendous forms of indigestion, and a severe form of bowel spasm called muco-membranous colitis where slithers of the lining of the bowel sloughed off and was excreted with the feces. The problem developed over many years, and was not evident when the women put their corset on, but subtly accrued afterwards, so most women didn’t recognise or believe the cause, and wanted to keep wearing corsets to keep up their attractive hour glass body appearance. However when corsets started going out of fashion the aliment declined in incidence and is now extremely rare. Wearing loose garments about the waist is a method of preventing, and relieving the condition.
2. Bending at the waist can cause and aggravate several abdominal ailments. For example, it can put additional strain on the abdominal muscles and wall, and aggravate any injuries in those places.
in the case of hiatus hernia where there is an injury or weakness in the hole in the diaphragm, bending can push part of the stomach through the hole into the chest, and cause pain by stretching that hole etc.
The stomach has a lining which usually protects it from acid, but the esophagus, or food pipe doesn’t, so bending can squeeze the stomach and push some acid up past a weak or injured stomach valve into the acid sensitive esophagus.
It can also produce additional pressure and push the displaced abdominal contents of visceroptosis even lower in the abdomen, and kink the loops of bowel to block the flow of digested material or cause colon spasm and pain.
Bending can also put pressure on any air in the stomach or colon, so avoid foods which are likely to cause bloating such as peas, beans, cabbage, and peanuts.
3. If the lining of the stomach or food pipe is weak then it may be vulnerable to pain caused by stomach acid, and any additional acid in the food can make the problem worse. Fruits such as oranges and lemons, and their juices etc, which have a lot of acid in them should be avoided.
4. If the lining of the stomach and esophagus are weak, but not actually ulcerated or bleeding, the blood thinning agents can aggravate the problem and cause pain. Therefore avoid substances which are known to thin the blood such as onion, garlic, ginkgo, and aspirin.
5. Peppers and spicy foods can also aggravate sensitive stomachs, so avoid them.
6. Food travels from the mouth to the rectum through many metres of bowel, so if there is any partial obstruction it can cause pain. The obstruction can be cause by hard feces, especially if sections of the bowel are narrow due to spasm. Therefore introduce high fibre foods into your diet, because fibre passes from the stomach to the bowel and absorbs moisture to form a large soft sponge-like texture which passes more easily through the contracted sections of bowel, and can even relieve the spasm. An apple for example, may be hard when eaten, but is churned and dissolved in the stomach to become liquid and fibre. Bear in mind that eating one apple is unlikely to overcome a problem along the entire bowel, so it may be necessary to eat two or three apples a day for two weeks or more to notice a beneficial effect
Food moves through the bowel in waves called peristalsis which occur at four hour intervals, which is why some people get abdominal pain in the middle of the night – the pain is due to non-fibrous food which has been eaten in the previous day, reaching a constricted part of the bowel. Consequently, avoiding any factor that causes spasm during the day, and eating fibrous foods, and avoiding acidic or spicy foods can reduce or prevent that pain.
The Chronic Abdominal Pain Essay ©
Death by 1000 cuts without the death
I had chronic intermittent abdominal pain which had not responded to any form of treatment in any effective or lasting way, so I decided to study it myself in 1975. It took me 23 years of experimentation before I was finally able to relieve that pain in 1998, and the ideas and methods are subject to copyright, and I own that intellectual property. However, I have found recently that many people, some of whom are top international researchers, have breached my copyright by using the ideas without asking for my permission, or mentioning me as the source. Other people are now using my method to prevent or treat such problems in themselves, and to educate students and society. See my report here.
At the very least I require each and every person who writes, or talks about, or teaches other people, to mention my name as the developer, and in some instances they should gain a licence to do so, and pay me a fee.
*******
I had some problems with abdominal discomfort probably since the age of six when I was ill for several months with hepatitis, and I lost a lot of body weight. My physique changed from being a healthy looking child with a straight spine, to a thin and stooped seven year old due to the fact that my weakened muscles had resulted in my skeleton collapsing under it’s own body weight. However, I was not aware of that until many years later when I began to study my own problems and treat them myself.
I also had some abdominal discomfort as a teenager, but nothing obvious until I was about 22 years old. One day I finished my days work as a clerk and drove to a hotel where I had a very large meal which would have made my stomach full and heavy. I then drove to a gymnastics club, and when I entered the hall I did a head over heels jump called a handspring. My back was arched as my feet his the ground, and I felt a ripping sensation in my belly just below the lower tip of my breast bone. There was no actual pain, and I didn’t start bleeding from the mouth, so I continued to participate in the gym activities for the remainder of the evening. I assumed that I may have injured my internal anatomy, and that like all external cuts and bruises it would heel within a few minutes or days. See gymnastics here.
Scroll in an out of this diagram and see here
However, over next few years I was troubled by abdominal pain occurring when I worked at a desk as a clerk. I had numerous medical tests but it didn’t’ matter how mild or severe the pain was at the time, nothing was evident on x-rays. I was advised that it was due to cardiospasm (also called esophageal achalasia) which is an abnormal function of the valve like structure between the food pipe and stomach.
The pain had some obscure features which I was unable to clearly identify at that time, but it didn’t occur when I started work at 9 a.m. in the morning, but would gradually become evident and annoying after leaning forward repeatedly for about an hour, and would then get gradually worse throughout the day.
Eventually I was getting several other symptoms as well, in particular a type of fatigue or exhaustion, and was ultimately consulting a doctor every two weeks, but none of the medications had any benefit, and then I was prescribed barbiturates at progressively increasing doses.
When the side-effects of the drugs were becoming more of a problem than the ailments I decided that the only way to relieve the pain was to leave work. However, as nothing was evident on x-rays it was made clear to me that there was going to be a lot of difficulty getting compensation or a pension at such a young age, so I decided to resign without my entitlements to superannuation benefits of 40% of my current salary. I was so ill that I couldn’t even continue for another few months to get long service leave of 9 weeks holiday on full pay.
My future prospects were that I had to spend the remainder of my life living in abject poverty, or study the medical literature and try to identify the cause and determine a way of treating those problems myself.
The fact that the pain appeared to be aggravated by sitting at a desk and leaning forward to write meant that I would also have the pain when doing any sort of writing or book work such as reading medical texts, but I didn’t’t have any choice. I was hoping that the benefits would outweigh the damage.
I started by laying on my back on the lounge room carpet with a pillow under my head, and staring at the ceiling and thinking about what to do. I then purchased a small Reader’s Digest book on the A-Z of medicine, and began reading it at the rate of one word a day.
When I got to the D’s I saw a description of Da Costa’s syndrome which matched my symptoms of chest pains, breathlessness and fatigue, and kept going for the next few months until l got to the Z’s but I couldn’t find anything else (Apart from the main symptoms of that ailment, abdominal pain is often one of the other common ones). See my report here.
I also joined a fitness programme at a medical research institute to see if exercise could gradually overcome the fatigue.
Furthermore, I cut out some strips of paper 6 inches square, and put the name of each symptom on the top, and kept a record of anything which seemed to aggravate them. If leaning forward to tie up shoe laces aggravated the abdominal pain, I noted it on that paper, and if it happened again and again I would put a tick next to it each time. Within a few months or years it became evident that many of the symptoms were aggravated by a variety of factors which involved leaning forward.
From what I had been told the cause was a complete mystery to the medical profession so I started writing essays about my findings. I was aware that Henry Gray had described the details of every millimetre of the human body in his book Gray’s Anatomy, in order to make it easier to understand the human condition, and I was writing about the symptoms with similar details, relating to every second and every activity or event of every day, so that the medical profession could understand illness more accurately, and more correctly. Naturally I knew that there would be many ‘ignorant’, and ‘useless’ and shallow minded fools who would misrepresent that as the ‘morbid’ and ‘obsessive’ ‘preoccupation’ with ‘trivial’ ‘details’ as seen in ‘hypochondria’ which is regarded as a ‘mental illness’.
Nevertheless, it was either a matter of solving the problem myself, or continuing to suffer, so I described as many details as necessary without giving any regard to the ‘useless’ critics.
I sent my essays off to magazines and within a short time the Australasian Nurses Journal was publishing them consistently at the rate of one every three months, so it wasn’t necessary to send them anywhere else.
My method was to establish consistent and reliable facts and write a small essay about each symptom, which took about two weeks. During that time my abdominal pain would increase and persist, and take two weeks to subside, and when I was free of pain I would start another essay. I probably wrote about 30 essays in five years and about fifteen of them were published. One of the last essays was called “The Matter of Framework” which I have since referred to as The Posture Theory. See here.
Also during that time I tried to get a different form of employment which would not cause problems but it was difficult to find anything that did not involve leaning forward. I considered selling real estate but that involved reading and filling in several pages of fine print in the sales agreement, so it was not suitable. I also tried window cleaning but developed abdominal pain if I stretched upwards or sideways to clean high or wide windows, or dizziness if I had to bend down to clean low windows. I also managed to find some part time work selling items that only required a small receipt with a stamp for my own details, and the name and address of the customer, the item and cost, and a signature. However, after several months a state of severe exhaustion would gradually and insidiously accrue which made it not worth while continuing, and required several months of rest to recover.
Another thing that I did was to go to the beach at least once each summer, and run a short distance, perhaps five yards along the sand, and do a head over heels hand spring with my back arched. On each and every occasion, as my feet hit the sand with a thud, I would feel the gnawing soreness in my upper abdomen, in the exact spot where the abdominal pain was generally felt. It confirmed the fact that it was related to the injury in the gym many years earlier. I did that handspring every year for at least four years to assess if the injury was healing, but the fact that I felt that pain each time indicated that it was chronic, and probably never likely to heal. The problems I had with that pain when sitting at a desk and leaning forward were obviously due to postural pressure on that sore spot.
It is further likely that my spine and chest shape disposed to that injury, and the other symptoms, and that repeatedly leaning forward was making them worse.
By the time I had finished the posture essay, which essentially solved the mystery about the cause of the symptoms, I was ready to stop writing essays entirely, and continue to look for other ways of earning a living.
However, one day while I was walking in town I met a friend who I had formerly studied with at the Institute of Technology, and I told him about my ideas. He then told me about a friend of his who was in charge of a research institute and suggested that I contact him. When I met the manager he was an amiable person who thought that one of my ideas could be researched in his facilities, and suggested it to his cardiologists. He later advised me that they were too busy, and talked me into organising a project myself.
I didn’t’t want to do it because I knew that at the end of a three month project I would have to write a report and would become crippled with abdominal pain in the process.
Nevertheless I continued, and one of the first requirements was for me to send a letter to a politician to get ‘official’ approval and endorsement for the project, so I spent about 2 weeks considering what the write. I didn’t want to do that either, but when I was asked to do it I left a meeting, and as I walked past the receptionists desk I asked for some pieces of paper and a biro. She then directed me to a desk in another room. I wrote several pages of text in a few minutes and when I returned and asked her to type it she looked ‘astonished’ and asked me how I could write so much in such a short time. I told her that I just sat down and kept writing until it was finished, without telling her that I wanted to do it as quickly as possible and with as little abdominal pain as possible.
The project was approved and proceeded, and the results were entirely successful in every way, and I did have to write the report, and did become crippled with pain. As the pain was subsiding I was asked to continue the programme on a larger scale from 20 to 80 volunteers, which I did in the same manner. It was successful again, and confirmed the original findings, and then I was told that, in order to have a great influence on this subject around the world I would need to continue and build up the study to include 200 volunteers. I didn’t’t want to explain why I was leaving, but just left the project.
I also tried to get my report written by a staff member who had experience with writing research papers but they were too busy, so I sent my own version to two medical journals. One of them replied with the standard “Thank you for your paper, but it is not acceptable at this time”, and the other one gave me a letter of explanation saying that my study was valuable, but was not written in the appropriate medical journal format. Needless to say, it wasn’t accepted so I put it in my filing cabinet and left it there. See here.
I spent some time trying out various other forms of employment and in between times laying on my back in the lounge and listening to talk back radio.
Because of my knowledge of medicine I would occasionally listen to a variety of ‘scientific experts’ making comments about health problems, and it was obvious that they were telling lies to the public so I became a medical critic. I naturally assumed that their research was being funded by such organisations as the tobacco industry to say such things as ‘there is no scientific proof that cigarette smoking causes lung cancer’. In some other cases the experts would have been paid directly, or indirectly for reasons related to other causes and illnesses.
Over the next few years I probably wrote 300 letters to newspapers. Each of them were about 100 words, and a small number were larger. I had acquired a large vocabulary, so I could write them in a few minutes. More than 100 of them were published in local, state, interstate, or national newspapers.
A few years later I had some blood tests and a CAT scan and was diagnosed with cancer and given two months to live with no hope of a cure, so I had to make some decisions about what to do with my future.
Previously, when I was 25, I tried to solve my own problems because they didn’t show up on x-rays, and nobody else seemed to be taking the matter seriously, so I was confident that I could come up with better ideas than “nothing”.
However, in this instance my cancer was evident on every test they did, and the best scientists, and the top research institutes in the world were trying to cure it and failing, and since I am not an arrogant person I didn’t think that I could do better than them in only two months, so I didn’t even try. Apart from getting some information pamphlets from the National Cancer Council, I just did what the physicians told me to do.
I decided that the best way to occupy my remaining time was to write a book about posture and health and sell it to school and public libraries so that parents and teachers could recognise and prevent posture related health problems in their children and students.
Of Course, if my belly ache got worse and caused some more permanent damage, it wouldn’t matter because I would soon be dead anyway.
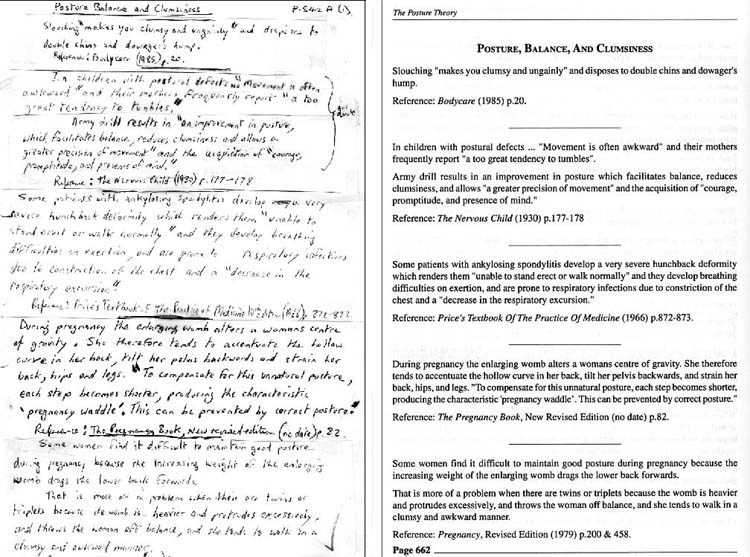
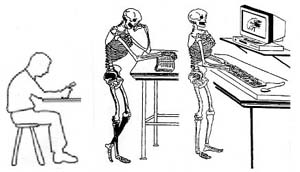
The left side of the illustration above shows a copy of the draft for a page in the 10th edition of my book.
I regularly avoided the pain that came from writing a whole page in one sitting by writing new lines, sentences, corrections, or diagrams on separate pieces of paper and cutting and pasting them in place with glue or sticky tape. In this example 6 pieces were used.
In previous editions I would take these drafts to a typist to prepare neatly.
However, I think from memory that I had probably learned to type by this edition, and added them straight into an Adobe publishing programme called Pagemaker, which can be seen in the right side of the illustration.
That programme has a feature which allows for the deletion of old material, and the replacement of new information anywhere in the page.
The draft copies for the 11th edition are all typed, so I assume that by then I had stopped handwriting entirely, and typed all of my new ideas directly into the computer.
One of my methods of research was to make observations of my own experience, and then look through the medical and other literature to see if other authors had made the same or similar observations, and would then add them as verification for the accuracy of the ideas
I proceeded to do a paragraph at a time, and add a sentence the next day, or a diagram the next, but as the book got larger I would need to edit each new 100 page section at the end of the year, so each year I would get quite severe abdominal pain and spend two or three months recovering. One year the pain was actually excruciating, and after several months it subsided, and I was left with a permanent change in abdominal function, but of course, as usual – nothing showed up on x-rays – or so I was told.
It was probably in the mid 1990’s that I considered the possiblity that adding a six inch high platform to my desk, to write on, might prevent the pain by reducing my tendency to lean forward, and I did get some slight benefit from it, and some time after that I added another six inch platform on top of that one, and then to write on a high table, or lecturn I then used an angled platform at the top to further reduce my need to lean forward, and that did reduce the abdominal pain, but it was still an occasional annoying problem.
I was able to publish the book economically by being one of the first people in Australia to use the new computer publishing facilities, but by 1998 the cost of typing and computing, and printing was becoming too expensive to continue. However, one day I was walking through the local library when I saw a computer with a “learn to type” programme on it so I started practicing. Within a short time I had purchased a typewriter, and then a computer, and the typing programme, and learned to type at the rate of fifteen minutes per day. I then purchased a computer publishing programme, and attended a course at a TAFE college to learn how to use it.
My hand writing speed of 20 words per minute became a typing speed of 60, increasing by 300%.
I soon started experimenting by putting my computer screen on top of platforms of various heights on my desk to bring it up to eye height so that I didn’t have to bend to read or write or type. Eventually I stopped sitting in a chair and started standing at the computer, and the abdominal pain subsided by 80 – 90%, and hasn’t been severe since.
Up until then my drafts consisted of strips of paper with sentences, paragraphs, pictures, and changes written by hand, which were wrtten or drawn in a few minutes, and later stuck together and re-arranged in logical order with sticky tape or glue, and then at the end of each year, were presented in neat printed text by a typist, and then a computer programmer. My books were bits and pieces of information put together in sections instead of paragraphs, with facts accessible from the table of contents and indexes, rather than continuous reading as a story or document.
My website was the same.
During the latter period I had two operations for cancer, and three types of chemotherapy for the cancer, which was finally cured by a stem cell transplant in the year 2000.
Also, when the 11th edition of my book passed 1000 pages I couldn’t afford to publish it, even though I was doing my own typing and computing.
I spent several years recovering from the side-effects of the chemotherapy, and was looking for other means of gaining an income, which included the buying and selling of second hand computers.
During that time a few friends started telling me about a new online encyclopedia called Wikipedia but I didn’t think anything about it until 2007 when I joined up to add free information. I soon learned that I couldn’t write about my own theory so I didn’t, until someone agreed to review it for me, with my co-operation to make it accurate.
When it was deleted I assumed that it was because some of the medical or related editors didn’t like their own ideas being challenged, because they shed doubt on the psychological cause, or they resented me for being a medical critic. I didn’t really care, because I had my own website anyway, and it was in the top ranking search engine page whereas, from what I knew, Wikipedia for that topic was insignificant or nonexistent.
However, when I started contributing to the topic of Da Costa’s syndrome I was continually being criticised by two editors working as a team in the most ridiculous and offensive manner. I have documented the massive number of lies they told elsewhere. See here and here.
Although I only added information about my own theory and research in the two months between December 2007 and January 2008, they spent the next 12 months setting up more than a dozen discussion pages in which they incessantly mentioned it, and linked to my website. They were obviously trying to create the illusion in the minds of other editors that they were continuously trying to stop me from pushing my theory into Wikpedia against the instructions from dozens of other editors.
They occasionally found an editor who believed their nonsense but those individuals didn’t know anything about the topic other than what they read in a dictionary, and some of them were sports editors who didn’t know anything about the subject, or teenagers who didn’t bother to check the facts.
As you can appreciate my two critics had read everything on my website, and they were describing my ideas as rubbish, while they or their anonymous associates were systematically transferring all of my ideas onto other pages to improve the status of Wikipedia articles. See my report here.
They would have also have read my book or been told about it and known that I experienced abdominal pain when I read or wrote, and exploited that problem by working as a team of two and writing thousands of words of criticism in response to my small number of contributions. They were obviously hoping that the pain of reading their nonsense and checking all of the facts, and reading thousands of words of policy in a short space of time would cripple me with pain and deter me from staying in Wikipedia.
However I dealt with that by ignoring their petty prattle and only contributing once per week on Sundays. Sometimes they would write so much derogatory tripe that I would also respond on the talk pages on a Tuesday or Wednesday.
In the first few months they spent a week collaborating against me in discussions spread over four pages and five thousand words, where I didn’t have the opportunity to reply, so after an administrator made a decision against me I spent a week preparing and writing a 2500 word response. Gordonofcartoon then deliberately mocked me by saying ‘cut this readable length’, to imply that it was too long to read, and he couldn’t be bothered responding. He knew that I would have had some pain for a week, and he was gloating about it by dismissing it with a sentence that took him ten seconds to write.
After deriding me to give other editors the idea that I was a worthless ‘newbie’ another editor responded in a patronising way by saying ‘at least he provided diffs’ (i.e. that I spent time looking through policies, and finding links to the evidence to verify that everything I said about them was true).
Later in the year they again wrote thousands of words of incessant criticism on an RFC page where they were trying to get other editors to delete an essay which I wrote about their tactics. During those discussions one of them used childish word play by making a snide remark of innuendo and double talk to imply that my reports of all of my pain in the past were all lies. This is what she wrote . . . “I think it would be fair to say that writing is not especially difficult for him, but perhaps we should not assume that it is trivial.“
Also, during those discussions, when I told the neutral editors that I would write a neutral essay outside Wikipedia, for them to check later, my two critics knew that it would take me several weeks to do properly so they arranged for an administrator (a sports editor) to block me before I finished it.
Gordonofcartoon was also selective in his choice of remarks. For example, when I wrote reports about his ill-mannered behaviour or gave examples of him deliberately breaking the rules of Wikipedia he would tell other editors that I was “continually griping (invariably lengthy)“, or “bellyaching“. e.g. here.
They used the same strategy on the arbitration page where Gordonofcartoon set it up and then wrote the first vindictive diatribe.
I then told the new group of editors that I would check on any other comments through the week and respond on Sunday, and then WhatamIdoing wrote an essay that was twice the length of mine, and filled it with lies, and then arranged for a friend of theirs to ban me on Thursday. See here.
What they didn’t understand is that when I stopped writing while sitting at a desk, and started typing, my writing speed increased three hundred percent, and when I started standing to type, my pain dropped by 90% in intensity and duration.
The aftermath
I was happy to give information to Wikipedia once per week, but I was not going to spend all day every day giving it for free.
I was also not going to waste my time in written discussions with completely useless and utterly worthless fools.
I decided to deal with them after I was banned, as they say, in my own sweet way, in my own sweet time, bit by bit, fact by fact, evidence by evidence, and essay by essay.
In that process I have continued to experiment and develop methods of minimising that pain, although I still need to do it in an intermittent manner to prevent it from getting out of control again.
I am now at an age where it doesn’t really matter what I do, and in fact, I will be occupied more usefully criticising those two fools than any other task.
If I can get them both banned from Wikipedia, I will be doing that organisation, and the world, a favor.
Sliding hernias and the crazies
I can recall reading or hearing an interview with a woman (probably on radio), in which she described how she had severe abdominal pain and had consulted hundreds of doctors, and had numerous blood tests, x-rays and CAT scans. She said that she had been prescribed countless pills and potions, and been referred to psychiatrists, and been told by most of them that her pain was all in the mind. She had been advised that all she had to do was to think positive and occupy her mind with something else and the pain would go away. Eventually she was starting to believe that she was actually mad, or was going mad.
That went on for 20 years, and one day she had another x-ray which showed a medical condition that was diagnosed as ‘sliding hernia‘.
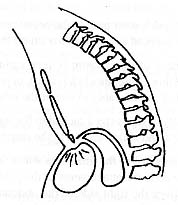
To understand that you will need to know that the chest and abdomen are separated by a broad flat muscle called the diaphragm, with the contents of the chest above it, and the abdominal organs below. There is a hole in it which allows the food pipe to pass through and enter the stomach immediately beneath.
Sometimes the muscular tissue around that hole is injured, or becomes weak, and sometimes a small portion of the stomach pushes up through it into the chest, and causes abdominal pain in that area. If it stays in the chest it shows up on an x-ray and can be diagnosed immediately as “hiatus hernia“. However, sometimes it slides in and out of the chest, in which case it is called a ‘sliding hernia’, and if the patient has an x-ray when the stomach is in the abdomen it appears to be perfectly normal. In some cases the ‘hernia’ goes undetected for many years, for that reason.
In that woman’s’ case the cause of her severe pain went undiagnosed, and unexplained for more than 20 years. She then had surgery to fix the problem, and recovered within a few weeks.
When she was later interviewed she reported how fortunate she was to have this mystery solved, because she could now lead a normal, happy, pain-free life, working, earning money, and going on holidays like everyone else, with a new future of prosperity to look forward to.
I then naturally expected her to say how much she understood the predicament of tens of millions of other people who had severe pain and had been undiagnosed, untreated, and wrongly labeled.
However. to my utter surprise she said that the greatest relief of all was that she was no longer put in the same category as those mental cases and crazies who whinge about trivial pain, or who imagine or fake pain to get sympathy or money.
Her comments were an utter betrayal of the millions of other patients with real undetectable abdominal pain.
If medical consumers don’t recognise the importance of being united then their position is virtually hopeless.
For a YouTube video of sliding hernia see here
GERD, also called GORD
Gastroesophageal Reflux Disease
Esophgaeal achalasia and esophagitis
Food generally moves from the mouth, down the foodpipe, through a type of valve, into the stomach. The stomach contains acid which is strong enough to dissolve and digest meat etc. The lining of the stomach is tough enough to resist normal acid damage, but the food pipe is not, so the valve generally stops the acid from leaking backwards and upwards to cause pain which is known as reflux or heartburn and other symptoms, and which are now being called Gastroesophageal reflux disease, which is abbreviated to GERD or GORD. It occurs because the valve like muscle between the food pipe and stomach occasionally doesn’t close properly.
The following comments are my review of another website which discusses this topic . . .
“The risk factors for reflux include hiatal hernia (a condition in which part of the stomach moves above the diaphragm, which is the muscle that separates the chest and abdominal cavities)”. Another risk factor is pregnancy, and many medications such as Beta blockers, and some anti-anxiey drugs or sleeping tablets can make the symptoms worse. Various activities can make the symptoms worse such as bending or stooping (and) laying down, so avoid bending over or exercising after eating, and the symptoms sometimes occur at night in which case they may be prevented by tilting the head of the bed up six inches. Also avoid garments or belts that fit tightly around your waist.
The symptoms can also be aggravated by consuming spicy foods, and citric fruits or juices, so avoiding them is a useful means of preventing reoccurrences. Large meals can aggravate the symptoms so eating small meals is beneficial,
Complications of the untreated condition include inflammation of the esophagus, esophageal ulcer, stricture or narrowing of the esophagus, Barrett’s esophagus (a change in the lining of the esophagus that can increase the risk of cancer), bronchospasm (irritation and spasm of the airways due to acid).
Looking at the esophagus with an endoscope and obtaining a sample of esophagus tissue for examination (esophagoscopy with biopsy) may be recommended to diagnose Barrett’s esophagus.
That review is a summary of information on the PubMed Health website which was Reviewed by: A.D.A.M. Editorial Team: David Zieve, MD, MHA, and David R. Eltz. on 12-10-2010 – Previously reviewed by George F. Longstreth, MD, Department of Gastroenterology, Kaiser Permanente Medical Care Program, San Diego, California (8/1/2009). See here
Heartburn and GERD (Gastroesophageal Reflux Disease) 23-12-12
I am not accusing Dr.Oz of deliberately stealing my ideas to use on his TV show, but he is definitely using my ideas, so at this stage I am politely asking him to acknowledge the fact that I have been developing and promoting those ideas, when other people have not, and when other people have in fact been calling my ideas nonsense.
In 1975 I had problems with abdominal pain. One of the diagnosis was oesophageal achalasia which refers to failure of the valve at the top of the stomach to function properly. Consequently stomach acid can pass through and up into the food pipe (esophagus) and irritate its lining to cause heartburn. I was also told that the cause of my pain was unknown, and that my symptoms were generally regarded as not having a physical basis and were caused by psychological factors.
The medications were not relieving the pain so I began studying the problem myself and came to the conclusion the poor posture and leaning forward was compressing the stomach, and stretching and straining and weakening that valve, and forcing some of the digested material and acid up through it and into the food pipe. About fifteen years late I found information from the nineteenth century that women who wore corsets had severe abdominal pains which were attributed to pressure on their stomachs.
I have since received a lot of criticism of my ideas being nonsense and fringy kookery that is not supported by reliable medical science, particularly from 2 Wikipedia editors.
However, I now accuse the producers of the Dr. Oz TV show of inadvertently breeching my copyright since I have been promoting those ideas in my books and on my website, contrary to most other authorities.
In particular a guest on the Dr.Oz show said that the pressure from the contents of a full stomach could push upwards and force acid into the food pipe. (That is a cause which I have discussed many times, as well as the fact that the enlarging womb of pregnancy can have the same effect, and is essentially proof that the pressure of poor posture pushing downwards on the stomach could do exactly the same thing).
More blatantly the segment suggested that the pressure of tight belts and tight girdles, or similar items of clothing which compressed the waist could do the same thing.
See my reports on corset pressure here and corsets and abdominal pains here and my essays about posture have been published since the mid 1970’s
Another article on abdominal pain
In some cases of chronic abdominal pain, where there is no relationship to eating or bowel function, but where it is related to postures such as laying, sitting or standing, “the abdominal wall should be suspected as the source of pain.”
There is often a tender trigger point. “If tenderness is unchanged or increased when abdominal muscles are tensed (positive Carnett’s sign), the abdominal wall is the likely origin of pain” and “If hernia or structural disease is excluded, injection of a local anesthetic with or without a corticosteroid into the pain trigger point” can be used to diagnose the cause of the problem and relieve the pain.”
The abdominal wall as a source of pain has received little attention, and only a few reviews on the topic have been published in the last decade. However, physicians who consider abdominal wall pain in their patients often find it. “In fact, overlooking the abdominal wall as a source of pain can result in a prolonged, expensive, frustrating and dangerous evaluation.”
Where there is no evidence of disease processes in the internal organs, there may be some indication of abdominal wall pain which includes an area of tenderness that is no more than a few centimetres in diameter, in some cases no larger than a fingertip, and pressing on that trigger point can cause the pain to radiate to a broader area. In one study 91% of patients reported significant relief of pain when a local anaesthetic was injected into that area. The identifiable causes included esophagitis, bile duct stricture, diverticular disease, inguirnal, femoral, and umbilical hernias, and unusual hernias such as epigastric hernia in the upper midline.‘
An example of this sort of problem was a 55 year old woman who had several episodes of pain during the course of one year, and “had undergone computed tomographic (CT) scanning of the abdomen, barium radiography and endoscopy of the digestive tract, and endoscopic retrograde cholangiopancreatography. The findings of these studies were normal.” i.e. despite all of those diagnostic procedures nothing could be found to explain her abdominal pain.”
A further comment was made about a condition labeled as “Idiopathic Abdominal Wall Pain” . . . “Many patients present with chronic pain that is not related to an identifiable mechanical or physiologic abnormality in the abdominal wall. Dealing with this ambiguous situation is somewhat similar to dealing with nonspecific low back pain, in that the exact structures and mechanisms responsible for the pain are often not known.”
“Pain trigger points frequently seem to lie along the lateral margins of the rectus abdominis muscles (linea semilunaris), where cutaneous nerve roots pass around the rectus sheath. It has been proposed that cutaneous nerve roots can become injured where they pass through the abdominal wall, perhaps by the stretching or compression of the nerve root along its course through the abdominal fascia.”
In some cases a tight belt or poorly fitted clothing can be aggravating the problem, and sometimes the xiphoid cartilage (the lower tip of the breastbone) is “the specific focus of pain.”
Reference: SAUD SULEIMAN, M.D. and DAVID E. JOHNSTON, M.D. August 2001, The Abdominal Wall: An Overlooked Source of Pain, Am Fam Physician.1;64(3):431-439. For more details see here
Median Arcuate Ligament Syndrome (MALS)
Another cause of abdominal pain which usually goes undetected
According to an article by Sam Montana on the Knoji website in January 2012, some people spend most of their lives suffering from intense abdominal pain which can occur at any time but mainly after meals. It may be caused by a condition called median arcuate ligament syndrome which usually goes undiagnosed because it is not evident on CAT scans, MRI’s, or blood tests.
Some patients are given medications which don’t relieve the symptoms and are often wrongly diagnosed with “Crohn ‘s disease, Irritable bowel syndrome”, “celiac disease”, or “Anorexia” or are told that the problem is “functional” or “all in their mind“, or related to mental problems, and that they will have to live with the intense pain and adjust their lives accordingly. In some cases the patients are passed onto psychologists by doctors who fail to diagnose the syndrome.
However their pain is actually caused by the median arcuate ligament compressing the celiac artery and impairing the blood flow through it. That ligament is “part of the diaphragm that connects the diaphragm with the vertebrae in the lumbar region between the ribs and the pelvis”. The problem is detected by “ultrasonography, Computed Tomography angiography (CT) and 3-D imaging” and it is treated by minor laparoscopic surgery to make small incisions in the stomach to cut the ligament. It results in complete relief of the pain, and the patients can return to normal living again with no further problems. See the full article by Sam Montana, and the description of the surgery performed by Dr. Donald Liu, M.D., Ph.D. of the University of Chicago here.
Undetectable chest pains
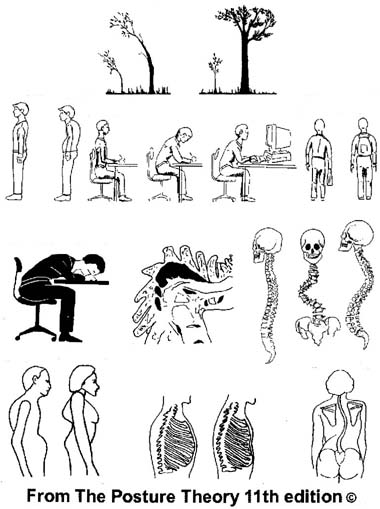
A comparison between the normal chest shape and the compressed ribs of a stooped physique can be seen in the illustration in the centre of the last row.
When I was young I would occasionally experience a sudden sharp stabbing or darting pain in the lower left side of my chest which felt as if someone had thrust a sewing needle through my skin to a depth of several inches. It only occurred about once every few months and would only last a fraction of a second, and although it was very distinct it was not particularly painful.
Many people experience such pains for no apparent reason when they are reading a newspaper or watching television, and because of it’s location it is common for them to worry that it might be due to some fault in their hearts.
The pain can also occur less frequently in the lower right side, or sometimes on both sides, or in other parts of the chest.
Nothing was evident on x-rays or other diagnostic tests, and I had never been given a satisfactory explanation for it so I eventually started looking for the cause myself and soon concluded from personal observation that it was indirectly associated with poor posture and leaning forward.
Poor posture places the head and shoulders forward, and the weight of them would be directed downwards along the front of the chest causing the ribs to be compressed together like the ribs of a piano accordion, and that could create an area of tenderness between them which occasionally produced the sudden sharp or twinging pains.
When I searched through the medical literature I found reports that some patients had a sense of soreness and weight in the area, without knowing or stating how that sensation occurred, but I assumed that it was due to the reasons that I have just stated which are related to poor posture. The pain was also reported as occurring when sitting or kneeling, or when bending and cranking the engine of a car. It could also occur at night, and then be relieved by getting up and moving about. It was also aggravated by the pressure from wearing tight clothing around the chest.
I also found that the tenderness is not noticed by most patients, but can be painful in others, and is usually confined to an area the size of a twenty cent piece, and that lightly dragging the head of a pin over the skin makes it sore, and finger pressure on that spot can aggravate it. The tenderness or pain is not affected by anesthetising the skin in the area, but it can be immediately relieved by injecting pain killing drugs into the muscle and fibrous tissue. That fact indicates that it has a real, and physical basis, and is located around and between the ribs.
When I was looking for confirmation of my own ideas I found reports that it was typically seen in patients who had stooped spines and long, narrow, or flat chests, and in his 1956 book Paul Wood suggested that the cause may be “faulty posture”. He also suggested another possibility that it may be caused by anxiety where an altered pattern of breathing puts strain on the diaphragm which in turn causes strain on the local muscles and the ribs attached to them.
However, as you can see many patients were not anxious at the time of the pain. They were usually sitting in a lounge chair and relaxing.
The diagnostic terminology for that symptom was “left-inframammary pain”, and would now also be called costo-chondritis.
I have also often felt another type of quite strong pain in the extreme left and right sides of my chest, and when I looked at books of anatomy it was clear that it was due to cramps in the long muscles on each side between the armpit and waist. Those pains have exactly the same characteristics as severe cramps in the calf muscles of the legs, although at times were worse. I attributed it to the fact that those muscles are designed for a normal shaped spine and chest, and that when structural differences are present the mechanical strain is excessive due to abnormal ‘leverage’. Those cramps could occur for no obvious reason, or could sometimes be brought on and aggravated by stretching my arms upwards or to the left or right, and by laughing for excessive periods of time which often occurred when I was practicing to be a stand up comedian.
References
Some of the information can be found in books where the authors try to distinguish the left inframammary pain from the symptoms of heart disease.
Reports which include the findings of physical aspects can be found in the second edition of a book called “Cardiac Symptoms in the Neuroses” by Dorothy Baker which was published by H.K.Lewis & Co. Ltd. London in 1955 . . .
and the second edition of a book called “Diseases of the Heart and Circulation” by Paul Wood which was published by Eyre and Spottiswoode in London in 1956 pages 937-947.
Undetectable Chronic Fatigue
The general opinion is that the standard medical examination does not reveal any physical or physiological evidence to confirm the diagnosis of chronic fatigue. However, such evidence is available in a thorough study of the research literature.
I also co-ordinated a study about chronic fatigue and found abnormalities in the response to exercise which can be seen here.
The invisible cause of itching
The cause of itching is invisible grass or tree pollens etc. which float about in the air. See my report here